All News

Debaters and moderators acknowledge IL6i may not be the only steroid sparing agents that would work for #GCA. Abatacept, secukinumab, JAKi are being evaluated #greatdebate @rheumnow #ACR23
TheDaoIndex KDAO2011 ( View Tweet)
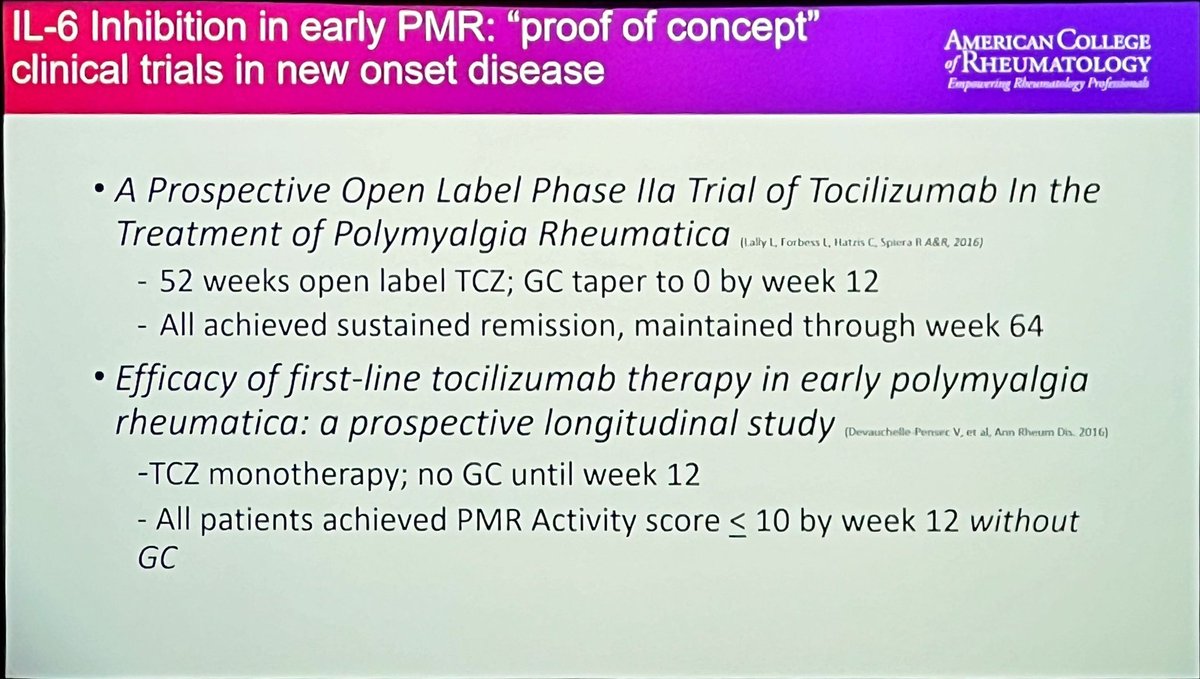
@philseo on why we SHOULD use IL-6i in GCA and PMR
1) Infection risk similar to TNFi
2) Too many (63%) pts remain on steroids at 1-2 yrs
3) May accelerate remission
4) Steroids are Bad, even at low doses
@RheumNow #ACR23 https://t.co/muPPcAc6LC
Robert B Chao, MD ( View Tweet)

More nuanced poll for #GreatDebate #ACR23
@RheumNow
How should we use biologics for PMR/GCA?
Eric Dein ( View Tweet)
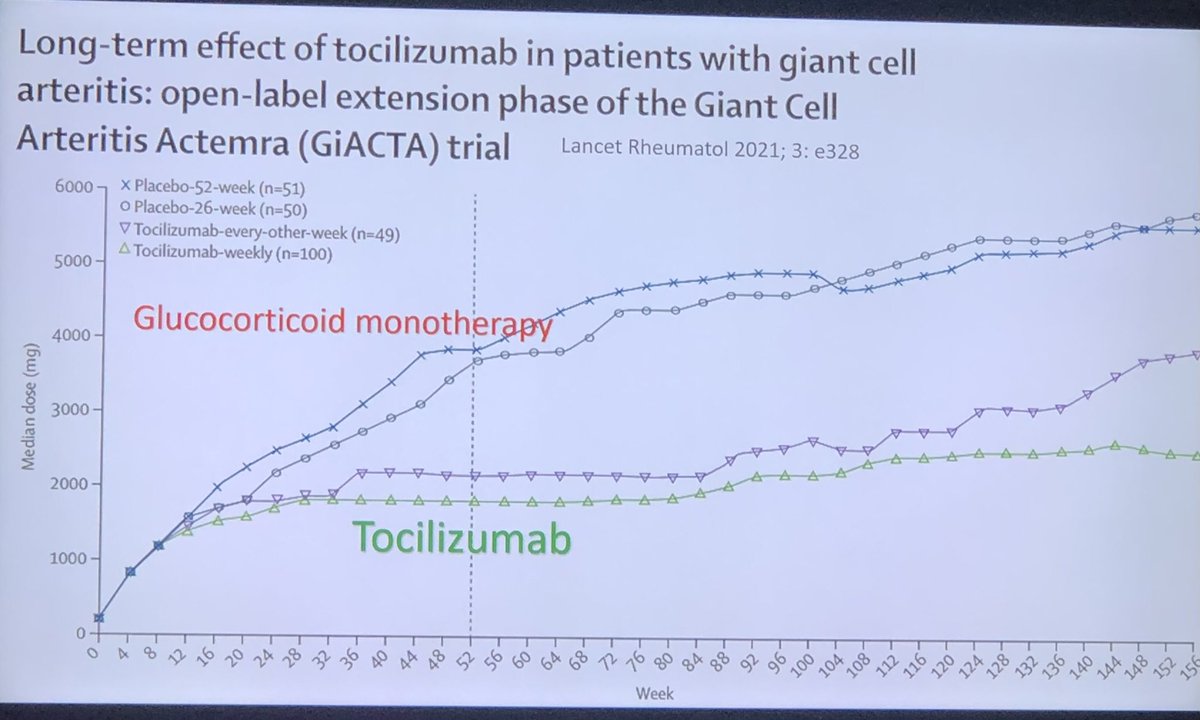
#GCA Rx #bDMARD is established to #steroid spare and reduce relapses. #Tocilizumab #GiACTA Dr Seo said ‘biologics work and steroids are bad!’ @ACRheum @RheumNow #ACR23 #ACRbest https://t.co/JmSE1KKlf5
Janet Pope ( View Tweet)
#GreatDebate #ACR23 @RheumNow
Advanced Rx 1st line in PMR/GCA
@philseo
IL-6 research in RA (STREAM, MOBILITY): safety of toci, sarilumab - compares to ADA
Ifn risk driven by GCs
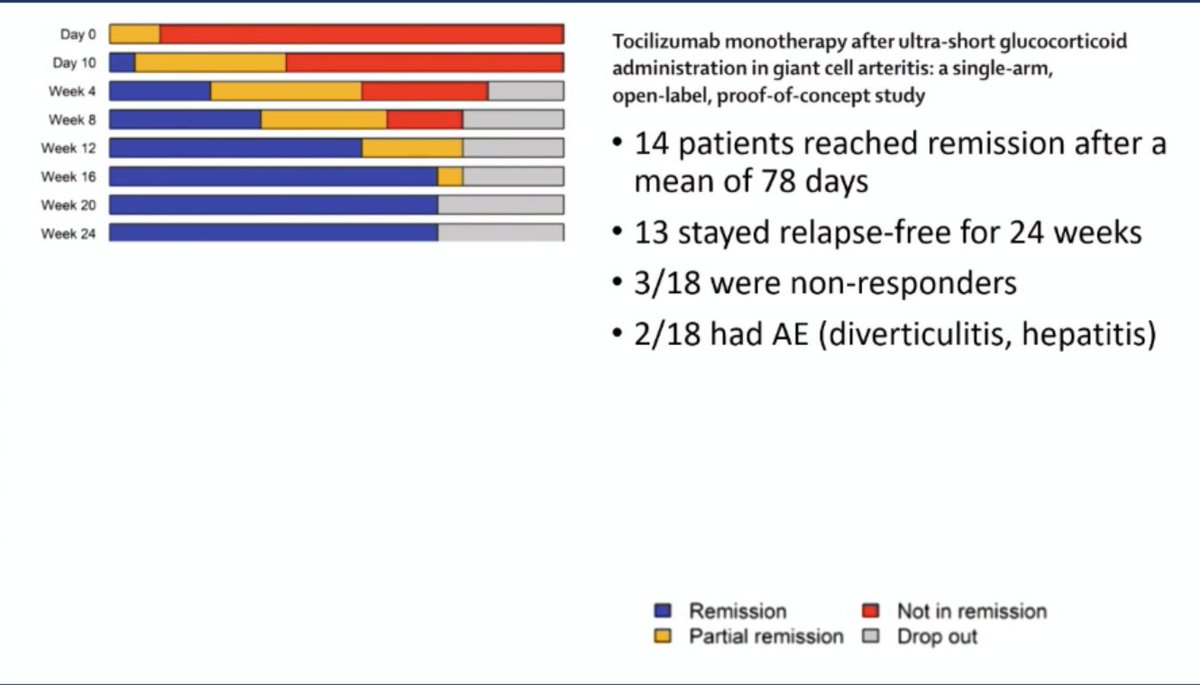
GUSTO: TCZ w/ only 3d GC pulse - 13/18 in remission 24, 52w
PMR: "its not just a little bit of pred" https://t.co/sAlQ0pttcq
Eric Dein ( View Tweet)
#GreatDebate #ACR23 @RheumNow
Advanced Rx 1st line in PMR/GCA?
@philseo: Yes
"Biologics work. Steroids suck" https://t.co/mQfbiaTsRV
Eric Dein ( View Tweet)
#ACR23 Great debate: should we use biologics at PMR/GCA onset?
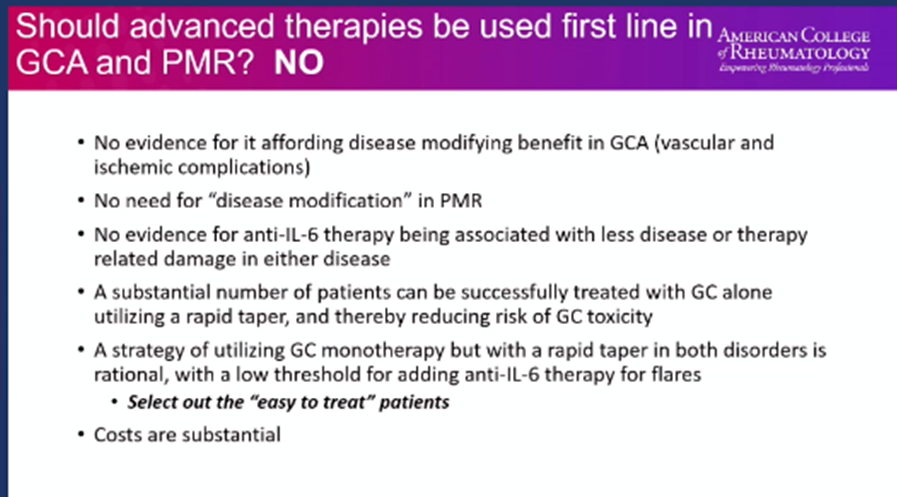
Dr Spiera (Cons)
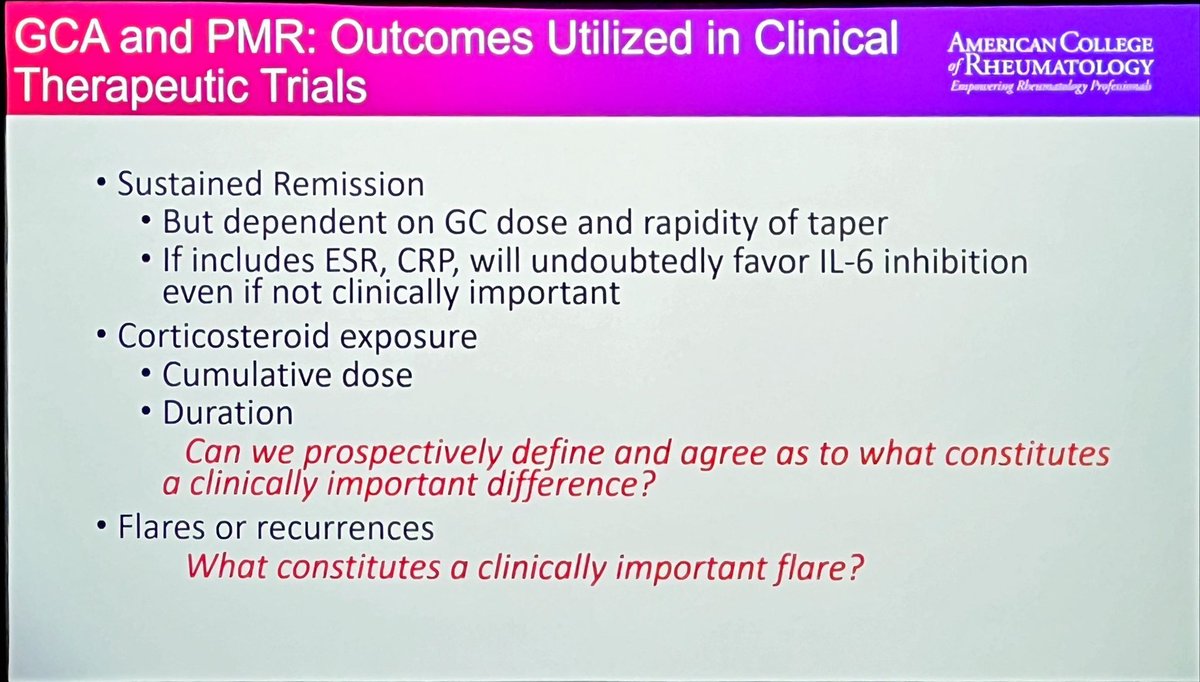
-Need to agree on clin important diff & flares
-No evidence as disease modifying in GCA
- No need for disease modifying in PMR
-Most pts can be treated with steroid & rapid taper
-Cost @RheumNow https://t.co/ptM8E7EQzF
Md Yuzaiful Md Yusof ( View Tweet)

The Great Debate #ACR23 - and it’s a cracker.
Is early steroid-sparing therapy justified in GCA/PMR? I don’t know, but Rob Spiera and @philseo will battle it out to tell us.
(and ably moderated by the always eloquent @SattuiSEMD)
I’ll put some highlights here ⬇️🧵
@RheumNow https://t.co/ASpuglyENv
David Liew drdavidliew ( View Tweet)
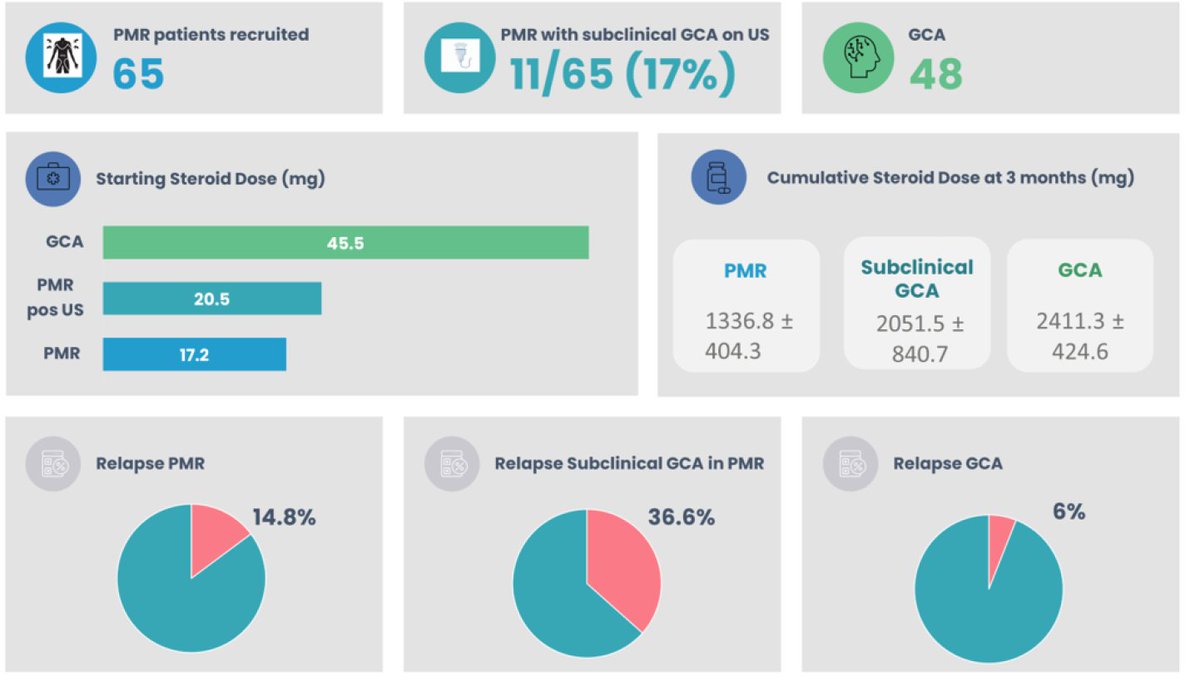
Baseline vascular ultrasound predicts clinical outcomes @ 3 months. Subclinical GCA = relapse 37% vs 15%. Higher cumulative steroid dose. @sharoncowley01 @DrTrishHarkins Abstr#1565 #ACR23 @RheumNow https://t.co/b35CkFS0lz https://t.co/suBGR1ByDK
Richard Conway ( View Tweet)
So firstly the no case, and Rob Spiera takes up the case, dictated by the electronic coin toss.
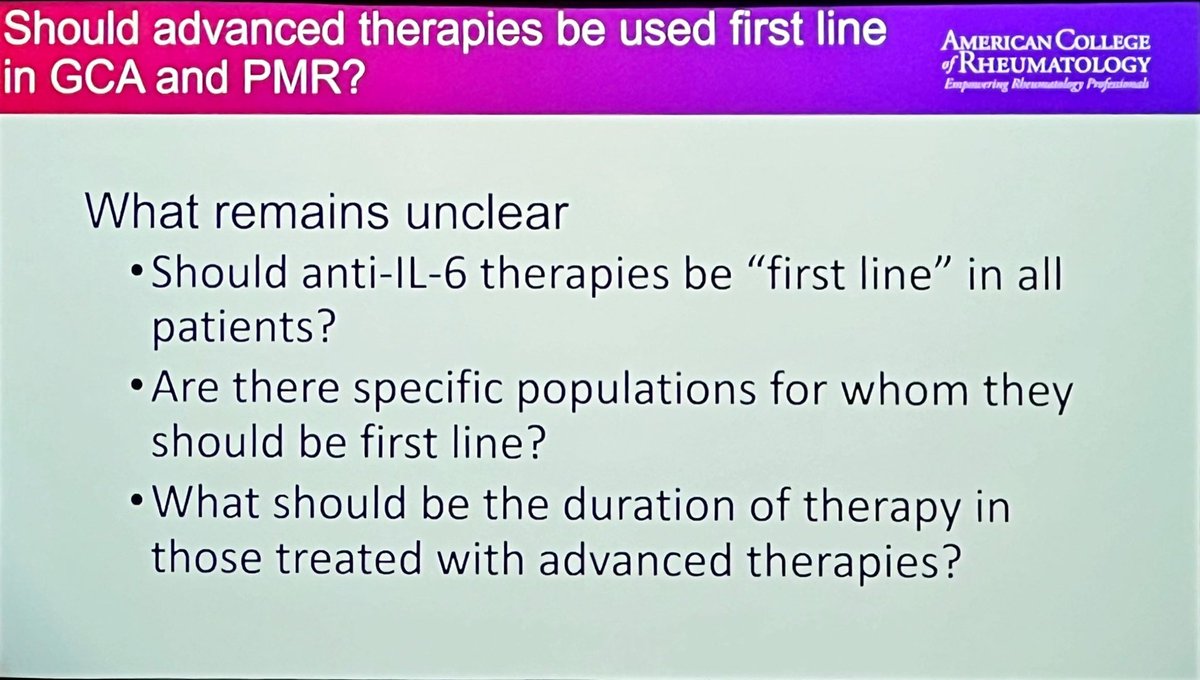
No-one disagrees that we need steroid-sparing options, or that IL-6Ri work in PMR and GCA. But it’s the strategy questions which remain in play:
#ACR23 @RheumNow https://t.co/I2QDU7l6DE
David Liew drdavidliew ( View Tweet)
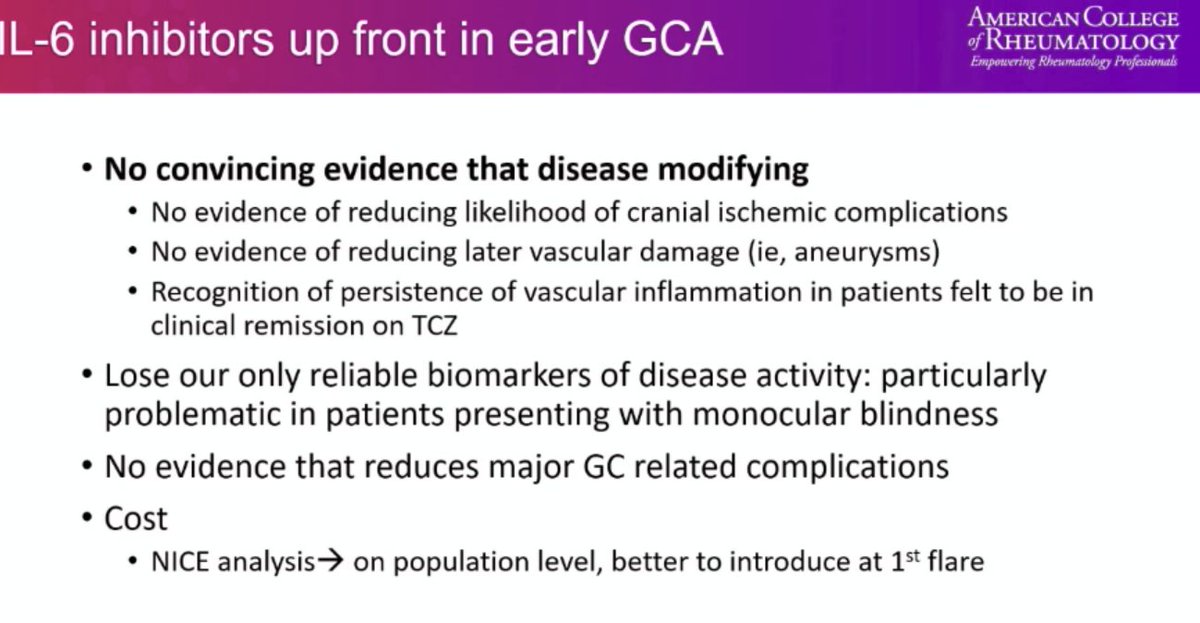
@RheumNow #ACR23 #GreatDebate
Use Advanced Rx for GCA 1st line?
Spiera: No
No ev for disease modification with early Rx
Lose only reliable biomark of dis activity w IL-6 inhib
No evid of reduced major GC AEs
$$
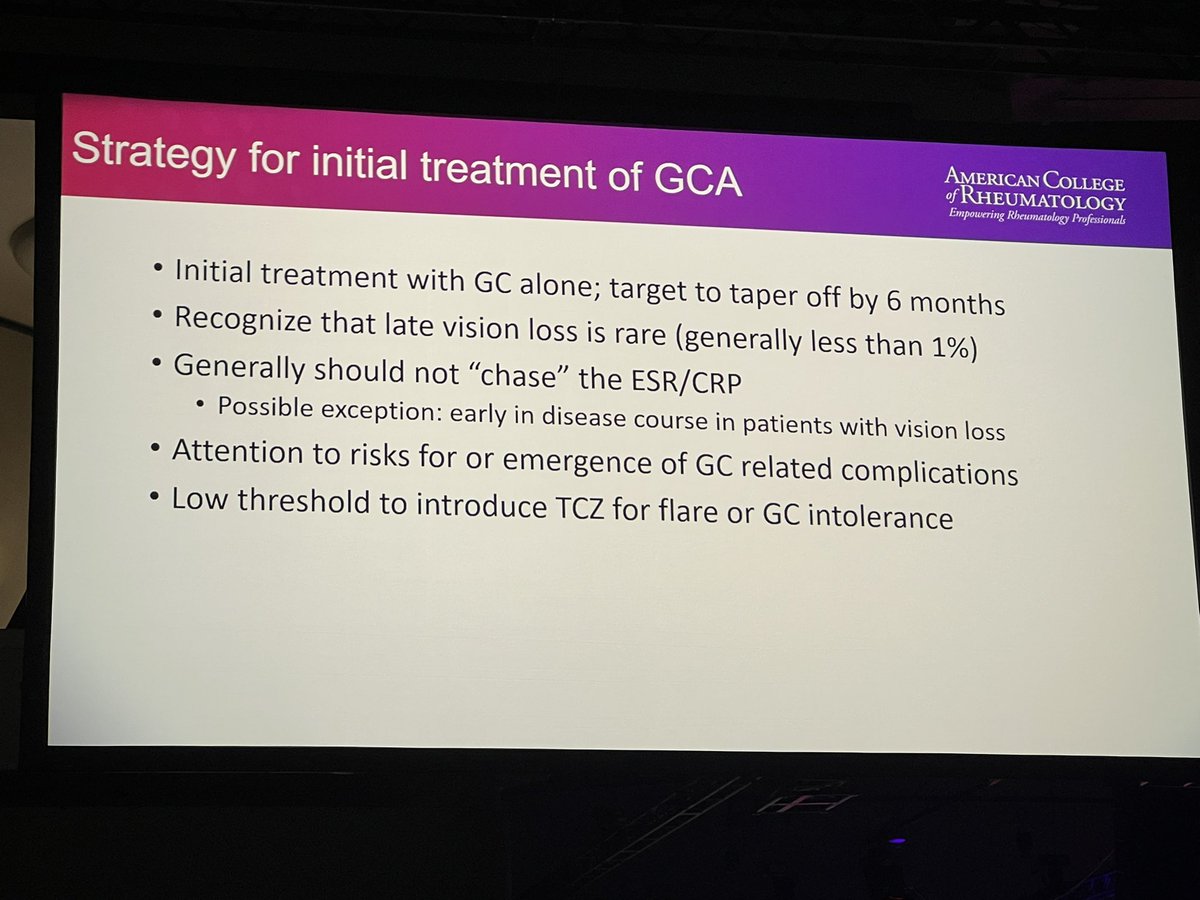
GCA: treat by GC alone, taper off by 6 m, low threshold to escal https://t.co/QxgAlVKitd
Eric Dein ( View Tweet)
@RheumNow So what might early steroid-sparing therapy in PMR/GCA achieve?
Cure? Superior disease activity control? Minimize damage? Improve QoL/function?
Well, sadly we have a long way to go in defining a lot of this:
#ACR23 @RheumNow https://t.co/QeidAHHm8x
David Liew drdavidliew ( View Tweet)
@RheumNow So in GCA, we don’t know if therapies can truly disease modify at all. There’s a lot of grumbling disease, and it’s unclear whether we can stop long-term vascular issues. And in PMR, we have very little data on early therapy at all.
So what’s the justification?
#ACR23 @RheumNow https://t.co/spAMqfSOy2
David Liew drdavidliew ( View Tweet)
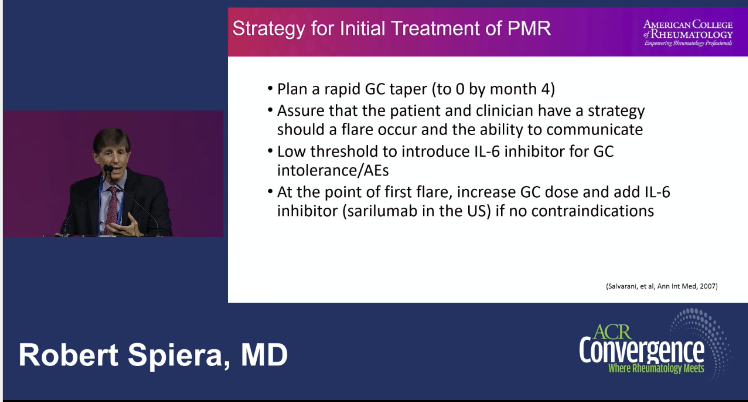
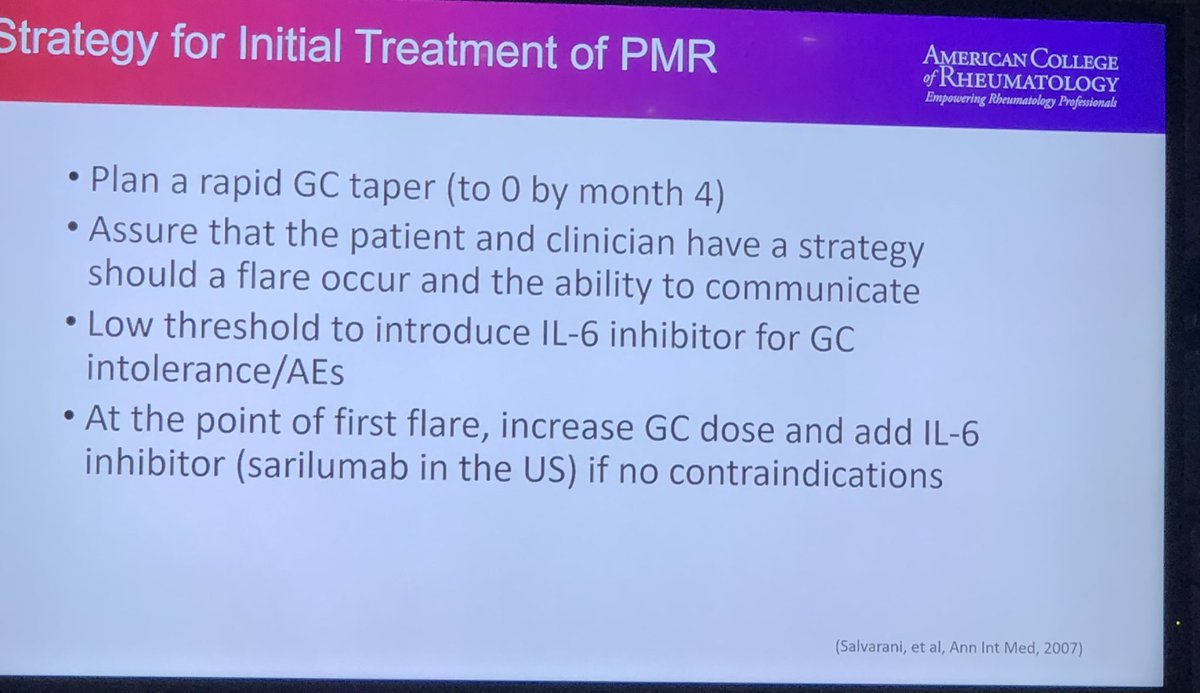
#ACR23 @RheumNow #GreatDebate
Treatment for PMR by Spiera
- Plan rapid GC taper. It is OK to flare, prepare pt!
- Low threshold to introduce anti-IL-6 for GC intolerance or AEs
No need for initial biologic treatment for PMR/GCA
@philseo rebuttal upcoming... https://t.co/A0f3b0fMOr
Eric Dein ( View Tweet)
Should IL-6i be first line in GCA/PMR? Dr. Spiera says steroids work, are cheap; no evidence of using IL6i early in disease. there had been cases where pts still had active vasculitis while on IL-6i. He starts with steroids first then add IL6i #GreatDebate #ACR23 @rheumnow https://t.co/Oq5Q9HFtW3
TheDaoIndex KDAO2011 ( View Tweet)
#ACR23 #Debate Dr Spiera says NO need to up front use #glucocorticoid #sparing drugs in PMR - maybe only if flaring. Esp in PMR vs #GCA where maybe bDMARD in GCA in some Pts (my opinion) but for sure if failing #ACRbest #ACR23 @RheumNow @ACRheum https://t.co/Rt7rGZv3fW
Janet Pope ( View Tweet)

1-Can we prevent RA ? Vagotomy?
2-CV events in auto immune rheumatic disease pregnancies.
3-CVS vasculitis , challenges and role of Brain biopsy
And others……..
https://t.co/BX8bDSX1M3
@RheumNow , daily recap
#ACR23
Nouf Al hemmadi ( View Tweet)
⭐️Real world data on use of #avacopan presented by @zach_wallace_md
#vasculitis
Important observations to inform the practice and management of #AAV https://t.co/gtZORcnt9t
KenWarringtonMD MdWarrington ( View Tweet)
Real-life data about the PEXIVAS reduced-dose glucocorticoid regimen in #granulomatosis with polyangiitis and microscopic #polyangiitis (Abstract 0725 https://t.co/7x34Hr0OMP)
@TerrierBen
#ACR23
#ACRambassador https://t.co/D8UfZvXQCl
Alessia Alunno ( View Tweet)

Reduced-dose GC regimen in severe GPA or MPS (creatinine >300 umol/L, RTX as induction) associated with increased risk of death, ESKD, progression before remission requiring treatment modification or relapse, Nagle S Abst#0725 #ACR23 #ACRBest @RheumNow https://t.co/ZVZYRnSy3n
Dr. Antoni Chan ( View Tweet)