Rheumatoid Arthritis

Caoilfhionn Connolly CaoilfhionnMD
1 year 8 months ago
📢 Late breaking #2002
➡️In ICI-induced arthritis, patients (n=100) report worsened pain, fatigue, & physical function vs population norms.
➡️High disease activity worsens symptoms
#acr24 @RheumNow @jhrheumatology

Antoni Chan MD (Prof) synovialjoints
1 year 8 months ago
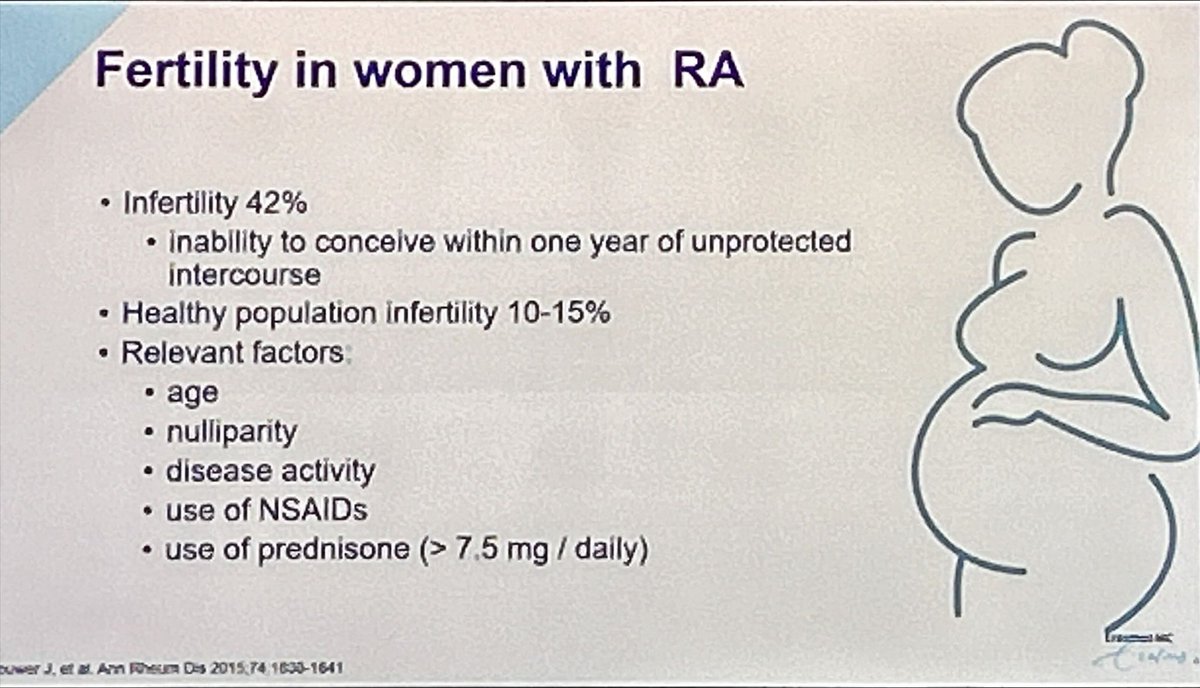
Fertility in RA. Improved outcomes in the T2T group. Abstr#1647 @RheumNow #ACR24 https://t.co/gLpY8enaEb
Dr. John Cush RheumNow
1 year 8 months ago
Shifting Trends in Initial RA Treatment Approaches
A recent study by Sparks et al (Abstract #0509) reveals evolving trends in disease-modifying antirheumatic drug (DMARD) usage for rheumatoid arthritis (RA) over two decades in the U.S.
https://t.co/6FN0WayZZR #ACR24 https://t.co/dc3CiNpKmx


David Liew drdavidliew
1 year 8 months ago
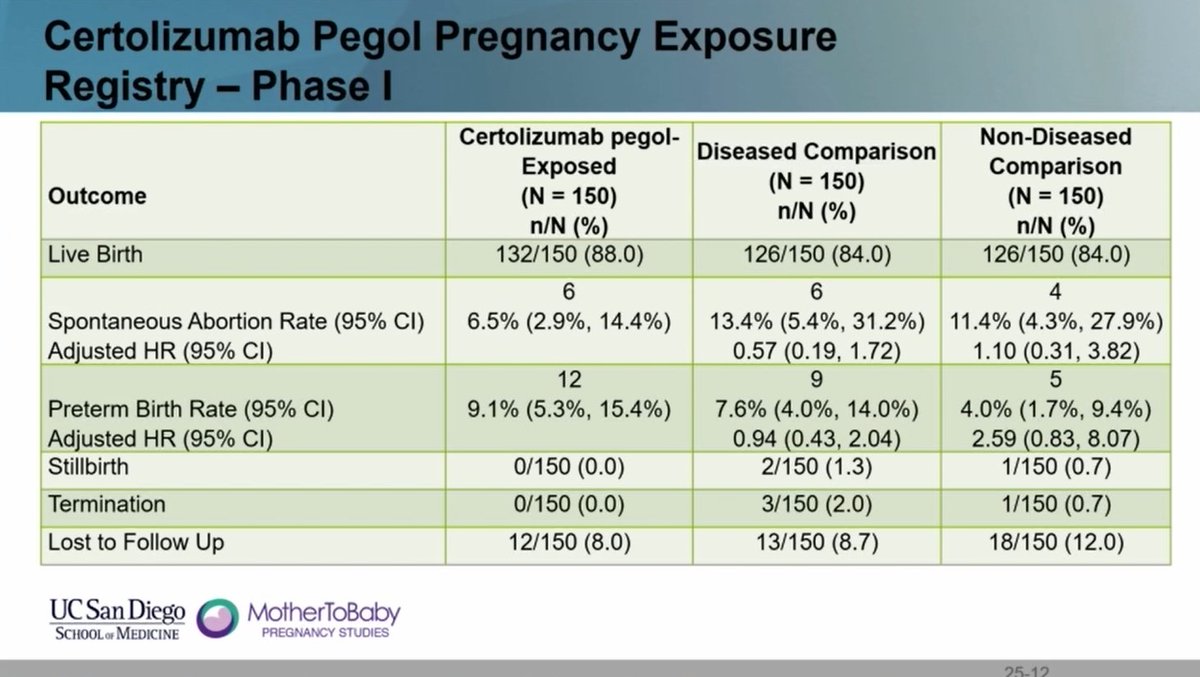
Nice data from the OTIS Autoimmune Disease in Pregnancy Project re: certolizumab-exposed pregnancies:
- spontaneous loss rate comparable to non-disease controls
- no stillbirths
- preterm similar to disease controls
Plenty positive for CZP in pregnancy!
#ACR24 ABST0805 @RheumNow https://t.co/XCRYsioxC0
Antoni Chan MD (Prof) synovialjoints
1 year 8 months ago
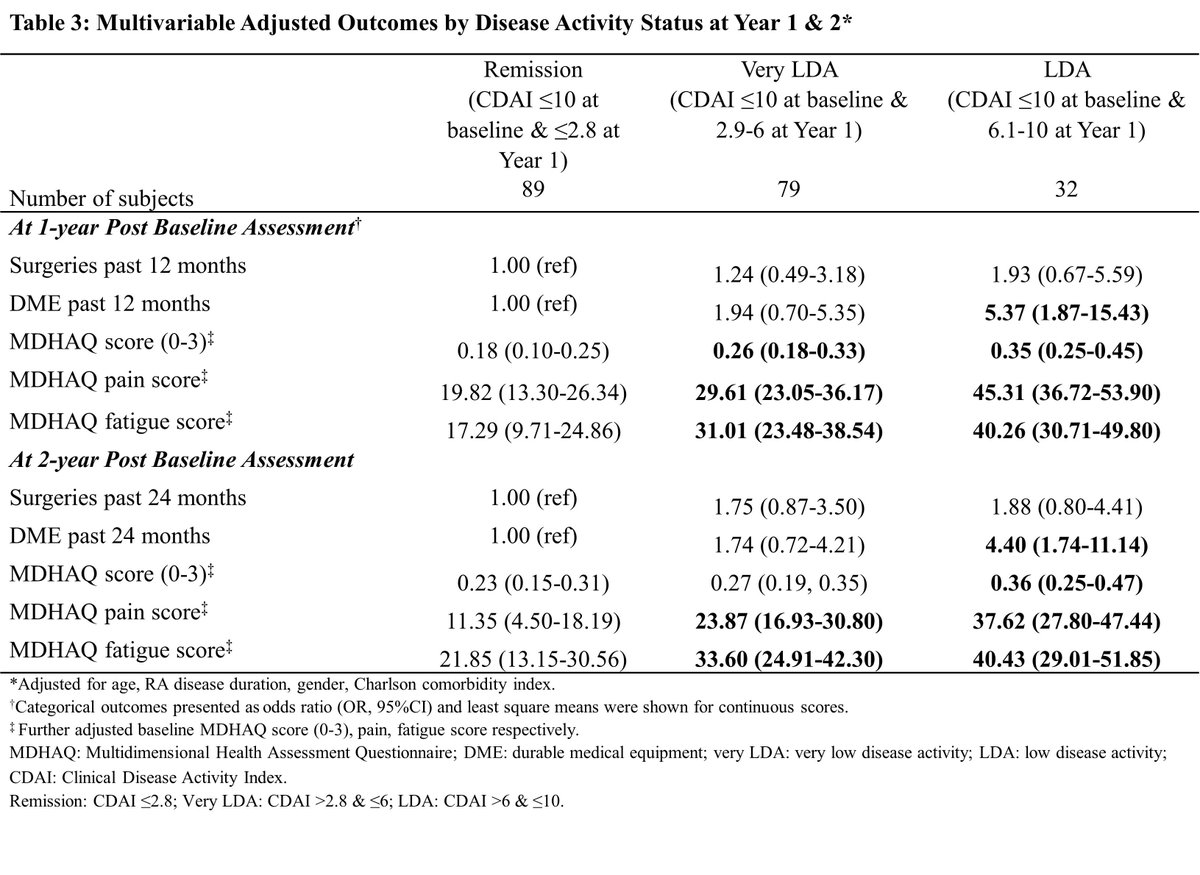
A study exploring the benefits of treating RA patients to remission after achieving low disease activity (LDA).
Key findings:
- Among patients initially at LDA, achieving remission (CDAI ≤2.8) led to significantly better functional outcomes and reduced durable medical equipment… https://t.co/SNPKlRieur https://t.co/YIQNMf3Oap
David Liew drdavidliew
1 year 8 months ago
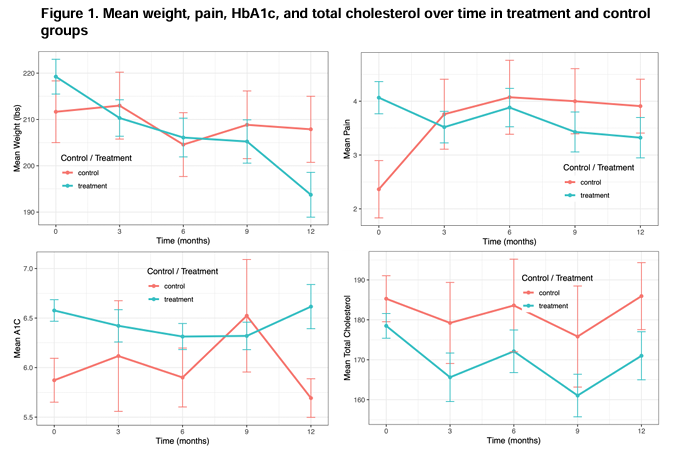
I have no doubt many of our RA patients will take GLP-1 agonists in the future.
Here's some data @UCLA showing significant differences in not just body weight and HbA1c, but pain.
Will be fascinating to see what it does for grumbling disease activity!
#ACR24 ABST2259 @RheumNow https://t.co/HdOPACEo3A

Mrinalini Dey DrMiniDey
1 year 8 months ago
What is #healthliteracy? Why is it important for our patients with #RMDs?
Come to poster 1913 today at #ACR24 to find out about health literacy & outcomes in #InflammatoryArthritis
For more information on this important topic, read my article @RheumNow
https://t.co/llWs5aYtpK

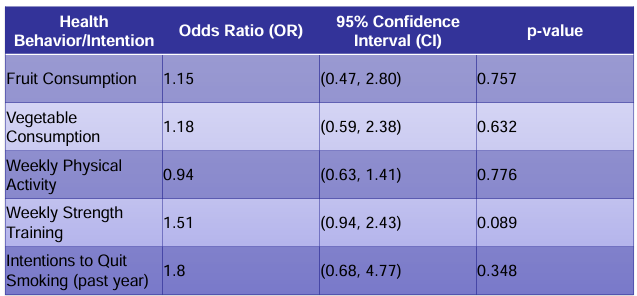
ORAL surveillance was a post-authorisation safety study of tofacitinib 5mg and 10mg versus TNF inhibitors, focusing on rates of adverse events, including MACE. A higher incidence of MACE was observed with the use of tofacitinib. Statins are recommended in patients with a history of atherosclerotic disease or 10 year predicted risk of MACE. But, how many patients with rheumatoid arthritis, at risk of MACE, are actually taking a statin?
David Liew drdavidliew
1 year 8 months ago
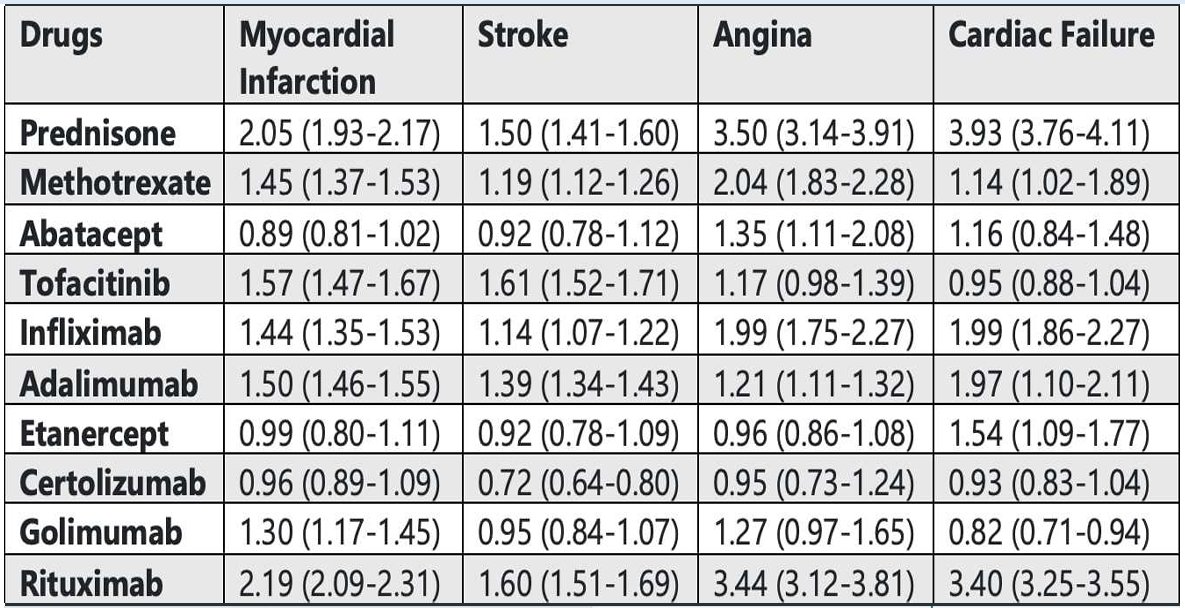
Instead of just JAKi, why don't we look at all our RA meds and MACE risk
FAERS data & reporting odds ratios here: all the caveats of voluntary reporting, so don't put too much weight, but...
prednisone. Don't forget pred is really not great for MACE!
#ACR24 ABST1981 @RheumNow https://t.co/L9SlPZF2Jd
David Liew drdavidliew
1 year 8 months ago
"There's an app for that"
but is it enough?
US informatics national survey 2017-18:
Rheum pts with digital health tools weren't any healthier living than those without (maybe helps exercise)
It might be a conversation starter, but it's only an adjunct
#ACR24 ABST1929 @RheumNow https://t.co/EZpSwm0zuP
David Liew drdavidliew
1 year 8 months ago
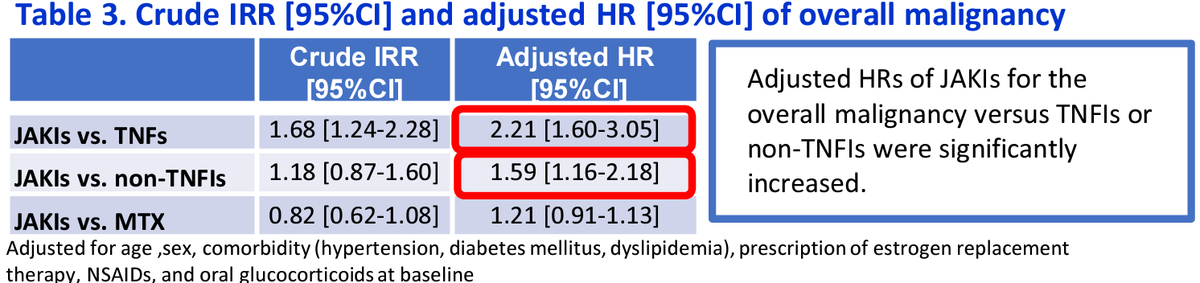
Always looking for cancer/CV signals from JAKi in big observational datasets w extensive JAKi use nationwide 🇯🇵 claims data RA pts n=52k (JAKi n=4.3k) Cancer with JAKi vs TNFi: aHR 2.2 (esp lung, lymphoma) This is a problem. Watch these data. #ACR24 ABST1336 @RheumNow #ACRBest https://t.co/vsnT46De6T
David Liew drdavidliew
1 year 8 months ago
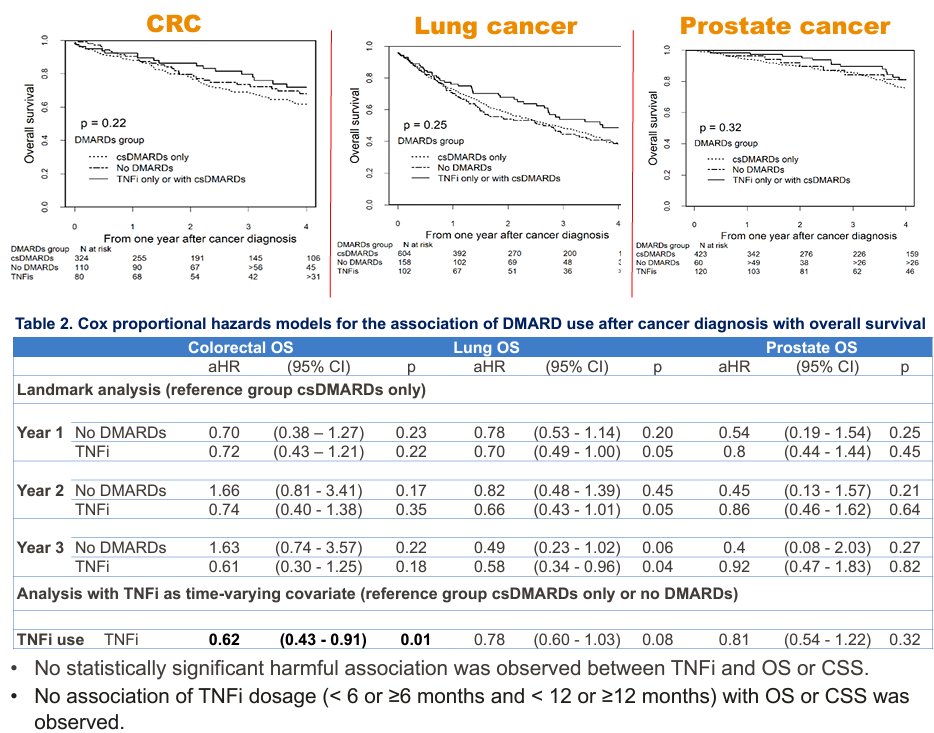
Should you worry about giving TNFi to RA pts after a cancer diagnosis?
Medicare data with colorectal, lung, prostate Ca:
TNFi pts survival no worse (numerically better) than csDMARDs
Cancer pts deserve good RA treatment!
#ACR24 ABST0202 Suarez-Almazor @MDAndersonNews @RheumNow https://t.co/w58MNqRt1T
David Liew drdavidliew
1 year 8 months ago
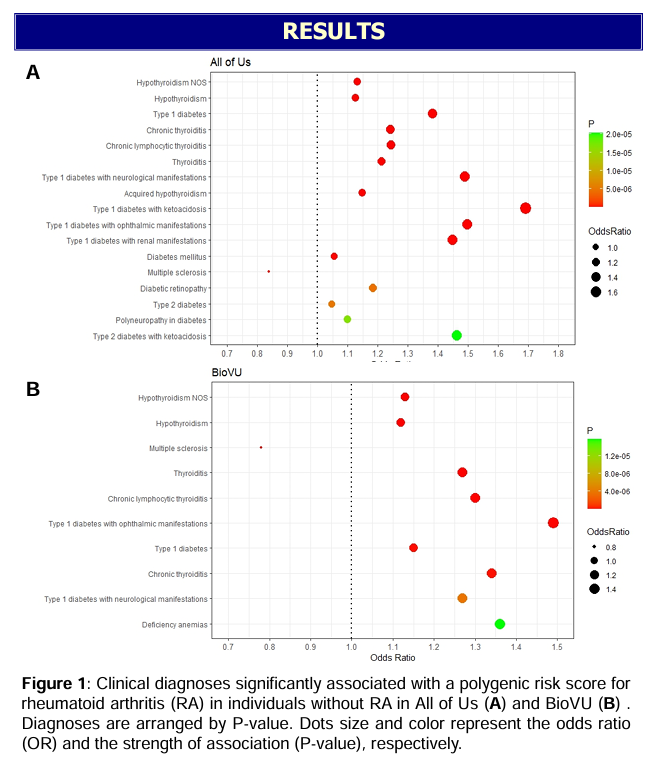
Now we have GWAS, we are getting polygenic risk scores for RA, and we can see what disease risks cluster with RA risk.
RA genetic risk clusters with risk for:
type 1 diabetes
thyroiditis
multiple sclerosis
What draws these diseases together?
#ACR24 ABST1365 @RheumNow https://t.co/28gU1nBEUG