Anti-Rheumatic Rx

The second day of EULAR 2021 took a big leap in online content. #EULAR2021 generated 2500 tweets yesterday. Here is a compilation (with links) of presentations were the “Best” as seen by our RheumNow faculty.


During Day 2 there were great sessions devoted to RA, spondylarthritis, fatigue and more. Here are some of my highlights from Day 2.


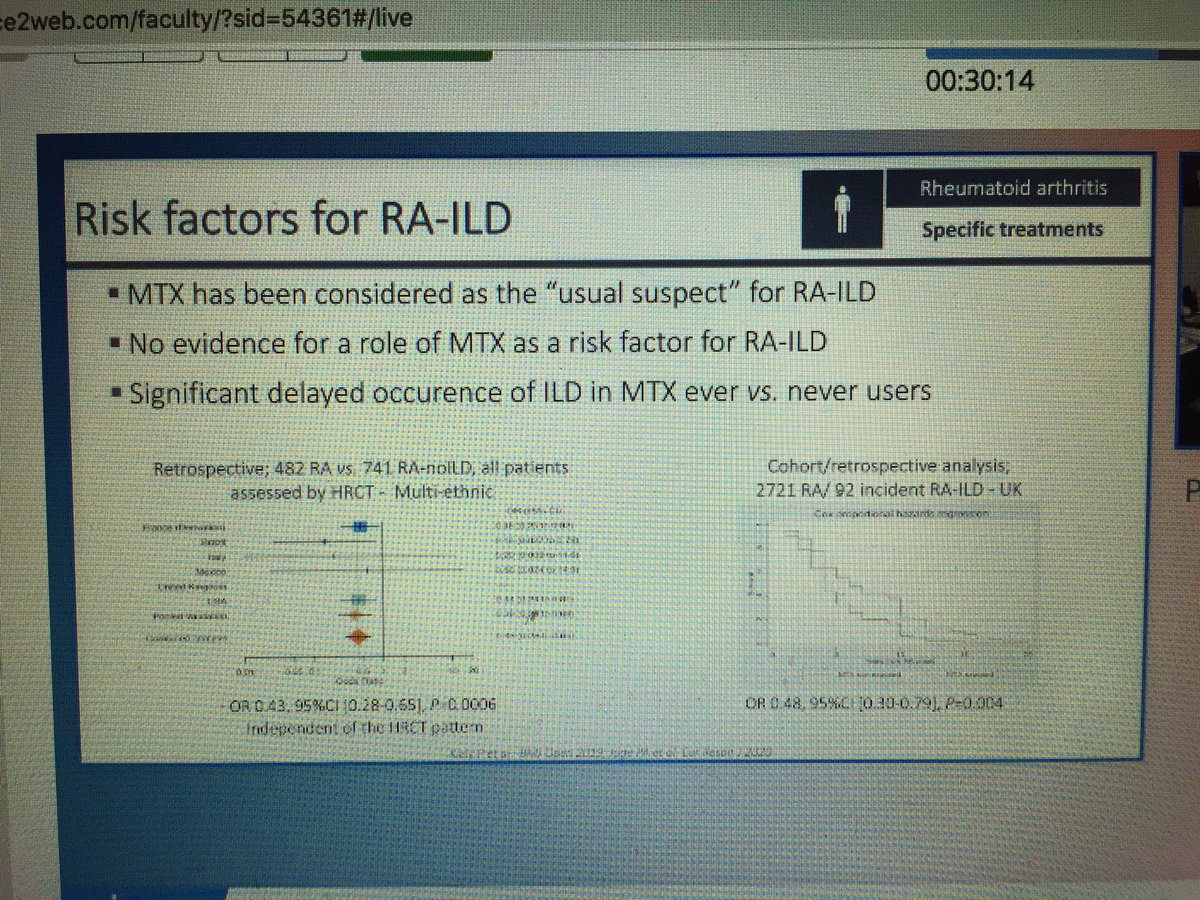
RA associated ILD (RA-ILD) is the most common extra-articular manifestation in RA. Its prevalence varies considerably, ranging from 5% to 30%, and is often underestimated since patients only become symptomatic or display abnormalities on chest X-Ray at a late stage of disease, leading to subsequent delay in diagnosis. In this context, several groups advocate for an earlier and more precise detection, using high resolution chest computed

Meral K. El Ramahi, MD MeralElRamahiMD
5 years 1 month ago
➡️COMPLETE-AS = obs study of bDMARD-naive Canadians w/ active AS tx w/ ADA or nbDMARDS/NSAID.
➡️> overall⬇️in dz burden & shorter time to achieve therapeutic response w/ ADA. But, ADA pts had higher b/l dz
OP0143 #EULAR2021 @RheumNow https://t.co/FpJmugsdVw

Robert B Chao, MD doctorRBC
5 years 1 month ago
⭐️All cancer excluding NMSC - 0.9HR TNFi vs cDMARD
⭐️Squamous cell CA - 1.2HR of TNFi vs cDMARD
⭐️No overall increase in all CA: RTX, TOCI
⭐️Abatacept 1.21HR for all cancer, mainly NMSC
⭐️needs more data on JAKs, IL-17, IL-23
Abs#6916
#EULAR2021 @RheumNow



Janet Pope Janetbirdope
5 years 1 month ago
Leave my MTX alone says pt & #rheumatologist if pt has chronic ILD. Acute pneumonia from MTX is NOT chronic ILD in RA @RheumNow @eular_org #EULAR2021 #BoehringerIngelheim RA ILD silent killer symposium https://t.co/IQTINuUpVq

Paul Studenic Stiddyo
5 years 1 month ago
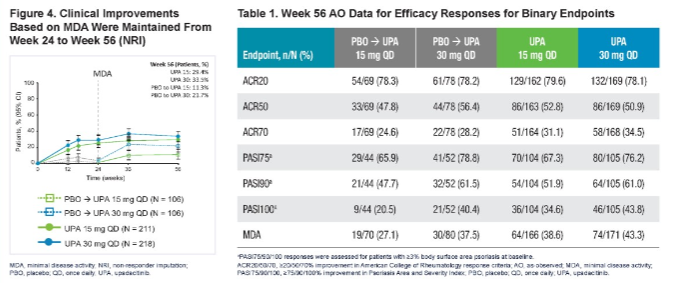
#POS0196 1 year results of the SELECT-PsA 2 study: Inadequate responders to ≥1bDMARD subjected to #upadacitinib maintained efficacy throughout week 56 (74% of pts completed 1-year)
#EULAR2021 @RheumNow https://t.co/xpqhzgeI6q

Eric Dein ejdein1
5 years 1 month ago
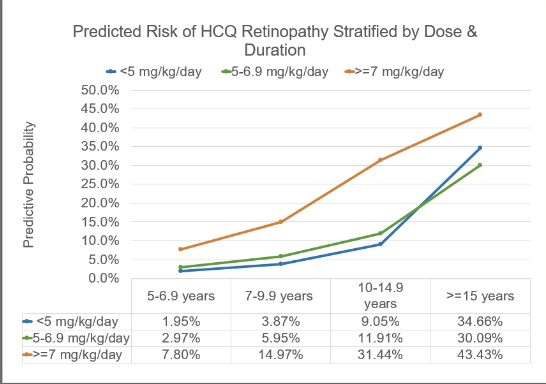
#EULAR2021 OP0133 retinal toxicity with HCQ use. ⬆️ risk:
⭐️Duration 10-14.9 yr (OR 5)
⭐️Duration >15 yr (OR 19)
⭐️Dose >7 mg/kg/d (OR 4.6)
⭐️Cum dose >2000 g
Atherosclerosis, age >80 seen in multi-var analysis
But didn't have HCQ levels to predict risk @MaxKonigMD
@RheumNow https://t.co/DzWWm0U64L

Dr. Antoni Chan synovialjoints
5 years 1 month ago
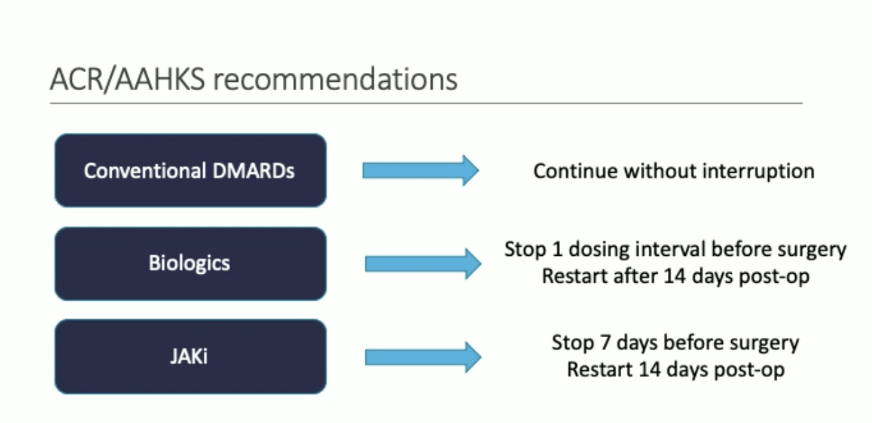
No requirement to stop cDMARDs before surgery. For biologics stop 1 dose before and restart 14 days post op, JAKi stop 7 days before, restart 14 days post op, glucocorticoids >10mg/day increases risk of infection in #rheumatoidarthritis Michael D George #EULAR2021
Eric Dein ejdein1
5 years 1 month ago
#EULAR Presentation 3478: Infection risk with surgeries:
⭐️Continue conventional DMARD
⭐️Some risk with biologics, may be confounder and no association with timing of infusions
⭐️Steroids are major risk factor! Esp >10 mg/d
⭐️Recommendations shown
⭐️Address other risks!
@rheumnow https://t.co/Bi02d4p9Mw

k dao KDAO2011
5 years 1 month ago
Based on the data, what would you do in a new SLE patient w/LN class IV who is already on a background of GC's+HCQ? @rheumnow @kidneydoc101 @Lupusreference






