

The Role of Calcineurin Inhibitors in Lupus Nephritis Save

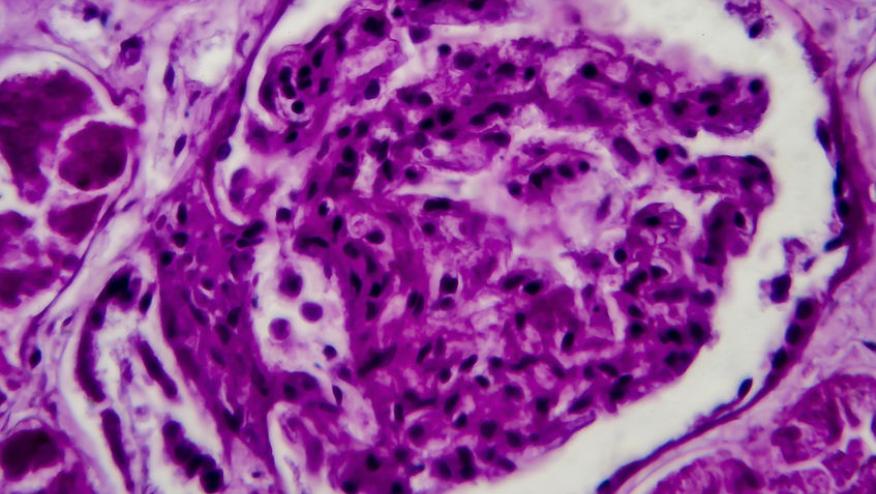
In the U.S, lupus nephritis affects approximately 40–50% of patients with systemic lupus erythematosus (SLE), contributing significantly to the morbidity and mortality of the affected individuals (1). However, significant differences in clinical approaches to lupus nephritis management still persist.
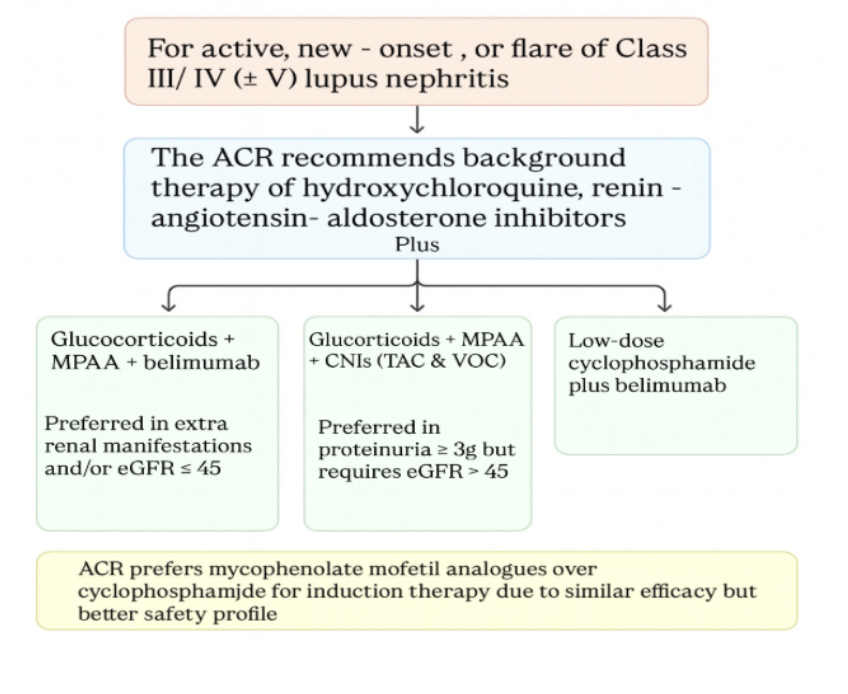
The release of the 2024 ACR guidelines for management of LN has significantly changed the approach towards early, aggressive immunosuppressive regimens with the introduction of the use of belimumab (BEL) or calcineurin inhibitors (CNIs) on a background of mycophenolic acid analogues (MPAA) and glucocorticoids (GC). Conventionally, GC and MPAA have been the cornerstone of managing active LN; however, large randomized controlled studies have shown superiority over dual immunosuppressive therapy by adding a third agent, such as voclosporin (VCS) or BEL, to achieve primary endpoints.
While CNIs historically have been recommended for use in other autoimmune inflammatory diseases (rheumatoid arthritis, psoriatic arthritis, etc), rheumatologists have been reluctant to prescribe them for lupus nephritis due to safety concerns, regimen complexity, or unfamiliarity.
Calcineurin Inhibitors: The New Kids on the Lupus Block?
Three calcineurin inhibitors, cyclosporine (CYA), tacrolimus (TAC), and voclosporin (VCS) have emerged as key agents in the contemporary management of lupus nephritis. Cyclosporin suppresses immunity by blocking T-cell activation and has podocyte-protective effects that reduce proteinuria in lupus nephritis; and relapses have been observed after discontinuation. Its use is further constrained by risks of nephrotoxicity.
Tacrolimus (TAC) has been extensively used for transplant immunosuppression for decades and works by blocking T-cell activation. By contrast, voclosporin (VCS) is a cyclosporine derivative with improved pharmacologic predictability, and was FDA-approved in 2021 for the management of active lupus nephritis.
The introduction of TAC and VCS as adjunct therapy in LN (III, IV, -/+V) patients has a dual mechanism of action: direct T cell-mediated immunosuppression; and an anti-proteinuric effect. The anti-proteinuric effect of CNIs is exerted by maintaining the podocyte cytoskeleton integrity and thus preventing podocyte effacement, the main culprit leading to proteinuria in patients with LN.
The AURORA trials (using background MPAA) demonstrated VCS efficacy in improving proteinuria as well as in achieving and maintaining renal response (complete/partial), while allowing for rapid steroid tapering (2,3).
Meanwhile, there are a few randomized controlled trials (RCTs) comparing the use of tacrolimus versus either MPAA or cyclophosphamide with the background of steroid taper. The TAC results revealed improvement in proteinuria, although pooled data from 3 RCTs showed substantial heterogeneity due to inconsistent background therapy and comparator (4,5,6). Additionally, most evidence for TAC use is limited to the Asian population.
Overall, the anti-proteinuric properties of CNIs distinguish them from other LN therapies. In the BLISS-LN trial, belimumab demonstrated no meaningful reduction in proteinuria among patients presenting with proteinuria of > 3g/day. Meanwhile, the latest ACR guidelines conditionally recommend triple therapy with MPAA and CNIs with glucocorticoid taper for patients with lupus nephritis and proteinuria ≥3 g/g (1).
Limitations
While CNIs should be avoided in patients with eGFR < eGFR ≤45 mL/min/1.73 m² due to risk of nephrotoxicity (1), belimumab (per the BLISS-LN trial) is efficacious in patients with GFR ≤45 mL/min/1.73 m² and extra-renal manifestations. Another concern might be the narrow therapeutic range of tacrolimus, requiring frequent drug monitoring. Conversely, VCS does not require drug monitoring for safety and/or therapeutic purposes.
To summarize, CNIs show significant promise for treating class III, IV, and ± V LN, based on the current data available, but there is a clear need for well-designed clinical trials to explore their efficacy, safety profile, and risk of relapse after medication discontinuation, given the limited long-term data available.
ACR 2024 guidelines for management of Lupus Nephritis:
References:
- 2024 American College of Rheumatology (ACR) Guideline for the Screening, Treatment, and Management of Lupus Nephritis.
Sammaritano LR, Askanase A, Bermas BL, et al. Arthritis & Rheumatology (Hoboken, N.J.). 2025. doi:10.1002/art.43212. - Efficacy and safety of voclosporin versus placebo for lupus nephritis (AURORA 1): a double-blind, randomised, multicentre, placebo-controlled, phase 3 trial.
Rovin BH, Teng YKO, Ginzler EM, et al.
Lancet (London, England). 2021;397(10289):2070-2080doi: 10.1016/S0140-6736(21)00578-X. - Safety and Efficacy of Long-Term Voclosporin Treatment for Lupus Nephritis in the Phase 3 AURORA 2 Clinical Trial.
Saxena A, Ginzler EM, Gibson K, et al.
Arthritis & Rheumatology (Hoboken, N.J.). 2024;76(1):59-67. doi:10.1002/art.42657. - Effect of Tacrolimus vs Intravenous Cyclophosphamide on Complete or Partial Response in Patients with Lupus Nephritis: A Randomized Clinical Trial.
Zheng Z, Zhang H, Peng X, et al. - Tacrolimus versus mycophenolate mofetil for induction therapy of lupus nephritis: a randomised controlled trial and long-term follow-up
Chi Chiu Mok et al. - Multitarget Therapy for Induction Treatment of Lupus Nephritis: A Randomized Trial
Zhihong Liu et al.
Join The Discussion
Do CNI improve survival rates and preserve renal function in patients with LN ?
Great question, CNIs did show improvement in complete renal response at 12 months based on the AURORA 1 trial but unfortunately we dont have data on long term improvement in renal response. We need more trials assessing long term outcomes including survival rate and renal response with use of CNIs in LN.






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.