What's New in Lyme Disease
JAMA has published an overview of new considerations on Lyme disease, focusing on Diagnostics, Vaccines, and Prevention.
Read Article
Search for Terms or Answers

JAMA has published an overview of new considerations on Lyme disease, focusing on Diagnostics, Vaccines, and Prevention.
Read Article
POETYK PsA-1 trial tested the disease modifying efficacy of deucravacitinib, a tyrosine kinase 2 (TYK2) inhibitor, in psoriatic arthritis (PsA) patients and was shown to be superior vs to placebo for clinical responses, patient-reported outcomes, and structural damage inhibition in PsA.
Read Article



Dr. Jack Cush reviews the news and recent journal reports on RheumNow.com.
Read Article

Eosinophilic granulomatosis with polyangiitis (EGPA) has long been managed by extrapolating results from microscopic polyangiitis and granulomatosis with polyangiitis clinical trials. But new insights into EGPA's has lead to advances in therapy and new treatment paradigms.
Read Article


People taking hydroxychloroquine (HCQ) for systemic lupus erythematosus (SLE) showed markedly increased risk for atherosclerotic cardiovascular disease when blood levels of the drug were low and when long-term adherence was poor, a prospective study showed.
Read Article
The rheumatology, genetics and NIH communities mourn for Dr. Daniel L. Kastner, who died on July 28, 2026, in Bethesda, Maryland, at age 74. The following are declarations, tributes, and memories dedicated to this mensch of a man, titan of science, memorable mentor and humble physician.
Read Article

A new review in the Journal of Cardiovascular Development and Disease (Tamirisa et al) synthesizes how systemic lupus erythematosus, rheumatoid arthritis, and systemic sclerosis have an increased risk of arrhythmias and sudden cardiac death attributable to shared immune pathways.
Read Article
The July 16th edition of JAMA reviews the highly prevalent problem of hip fractures - a major global health burden: 14.2 million occur worldwide annually (280,000 in the US), with global incidence higher in women (833.9/100,000) than men (510.0/100,000). Lifetime risk at age 50 is 22.9% for
Read Article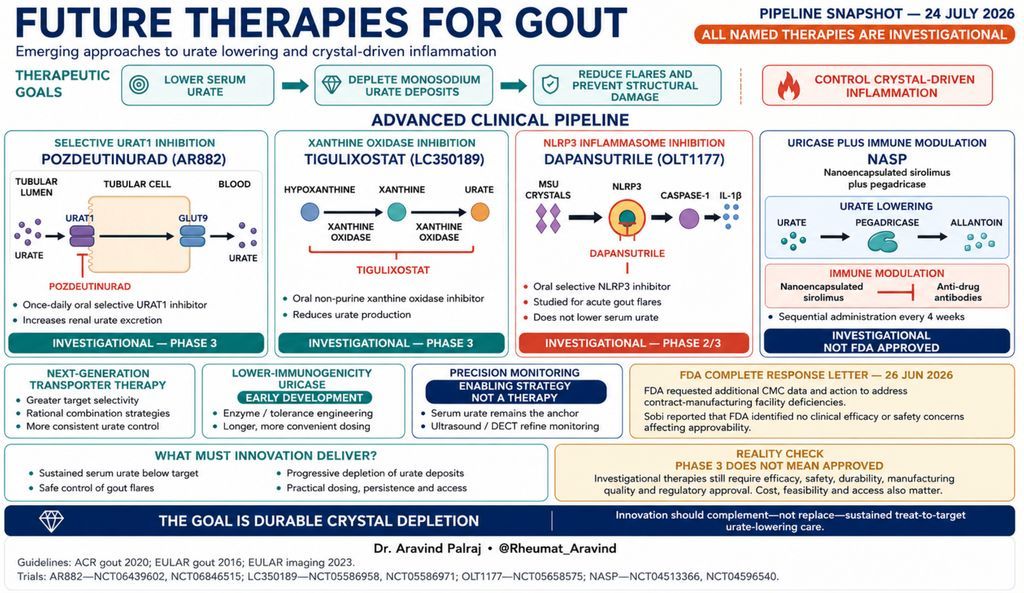

Dr. Jack Cush reviews the news and journal articles from this past week on RheumNow.com.
Read Article

During this month-long campaign on Gout, we have documented many significant changes in our approach to gout, as well as many unmet needs and deficiencies that merit our continued, primary attention. We are all familiar with the famous 1905 quote, “Those who cannot remember the past
Read Article

Rheumatologists are used to the concept of disease remission as this is a treatment goal we use for many chronic rheumatic diseases in our clinical practice. Recently, G-CAN (the Gout and Crystal Arthritis Network), endorsed a
Read Article
After data manipulation allegations, the FDA has been calling for the vasculitis drug to be pulled from the market since January.
Amgen has submitted a third-party review of avacopan's (Tavneos) pivotal trial data and other analyses to the FDA in a bid to keep the embattled drug for
Read Article



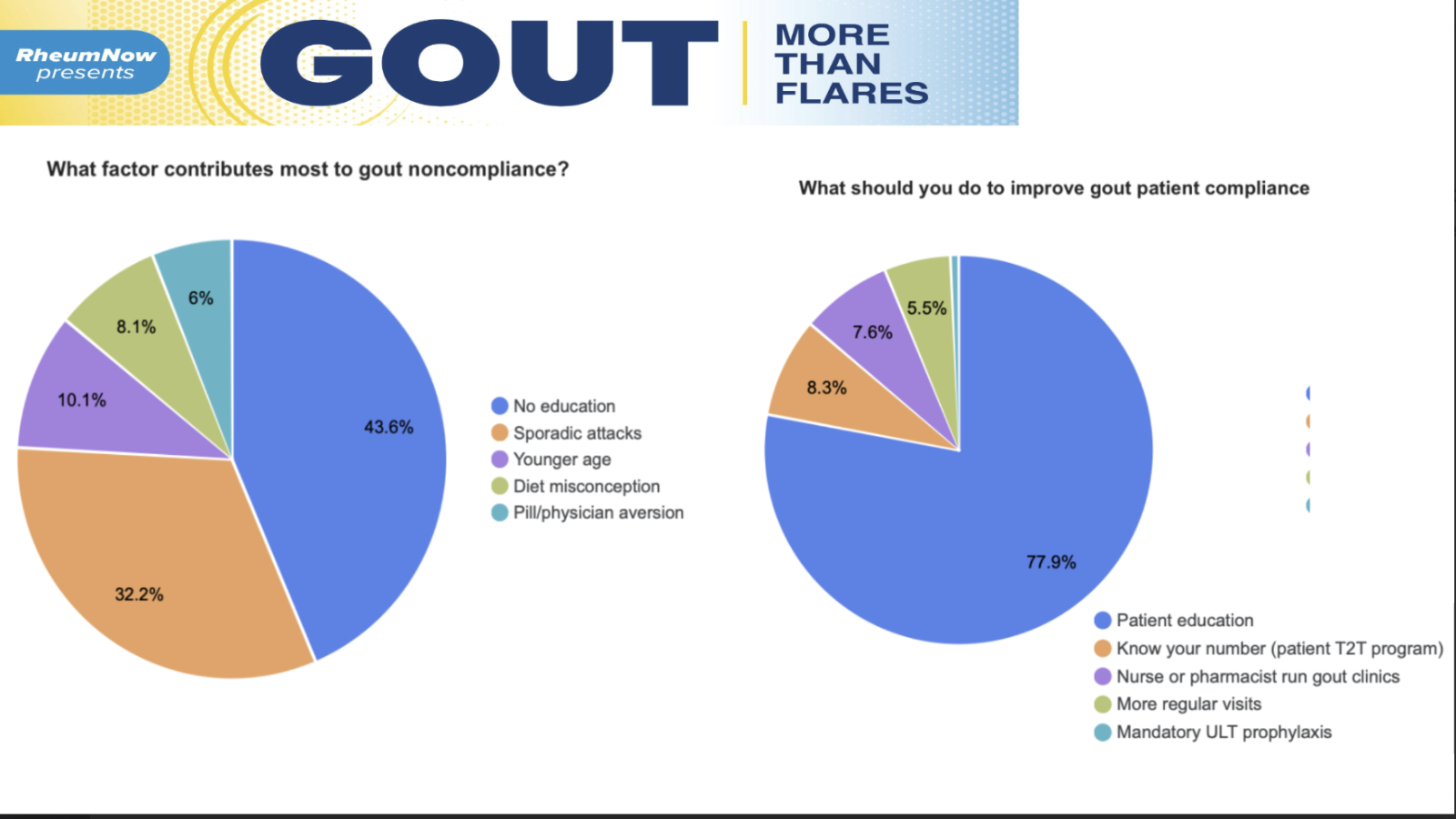
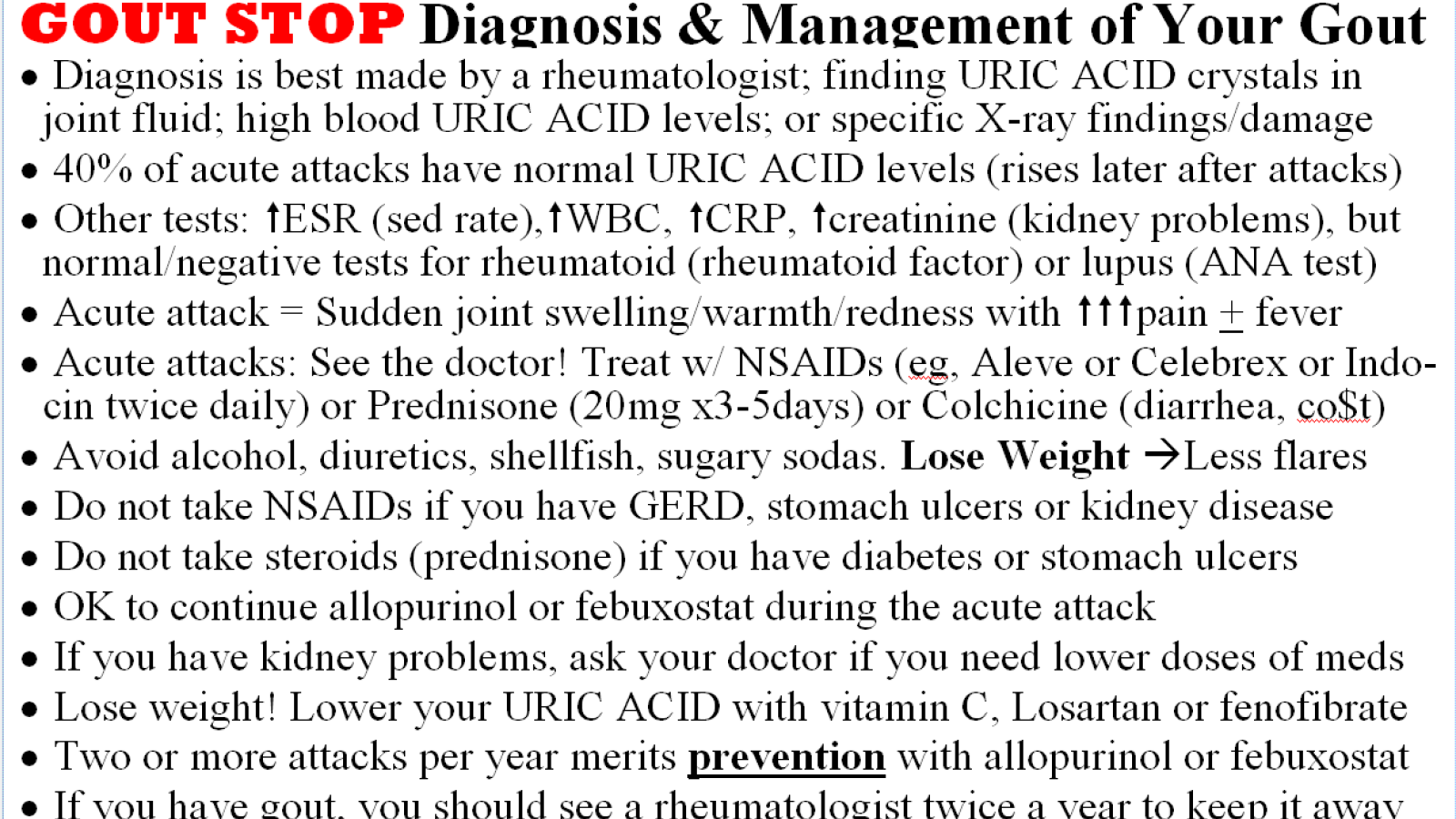
Dr. Jack Cush reviews Gout in this continuing series for Advanced Practice Rheum. Review the companion slide deck here.


By downloading this material, I acknowledge that it may be used only for personal use and personal education and that I will accredit RheumNow.com as the source and owner of this material. Commercial use or mass reproduction of this material without permission from RheumNow (info@rheumnow.com) is prohibited.