
Tweets
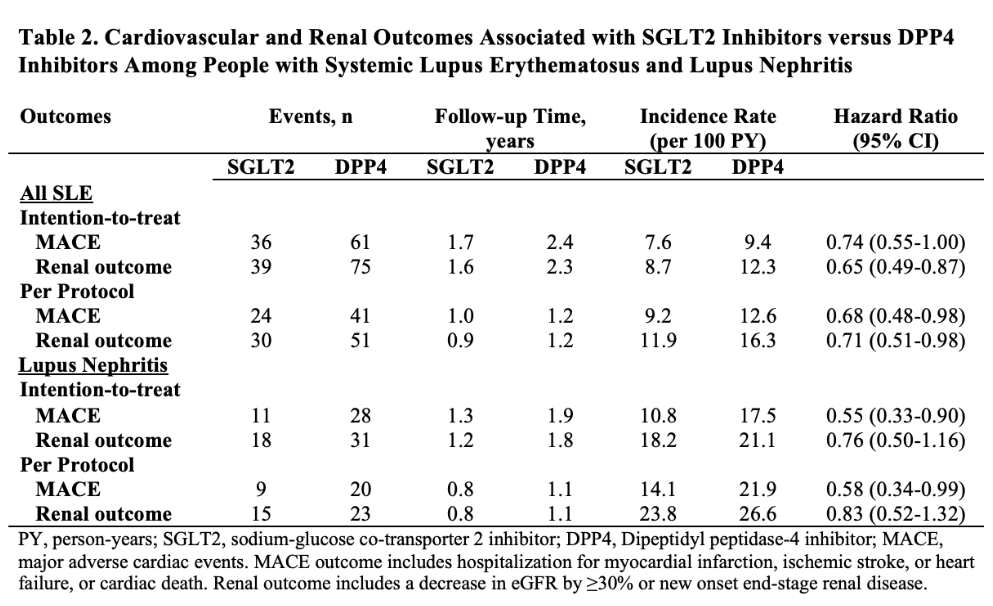
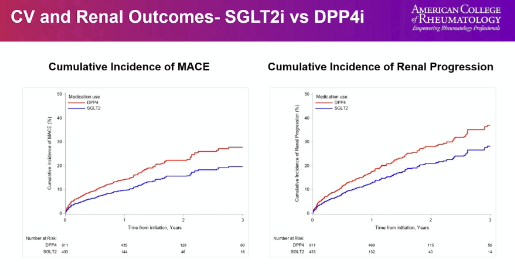
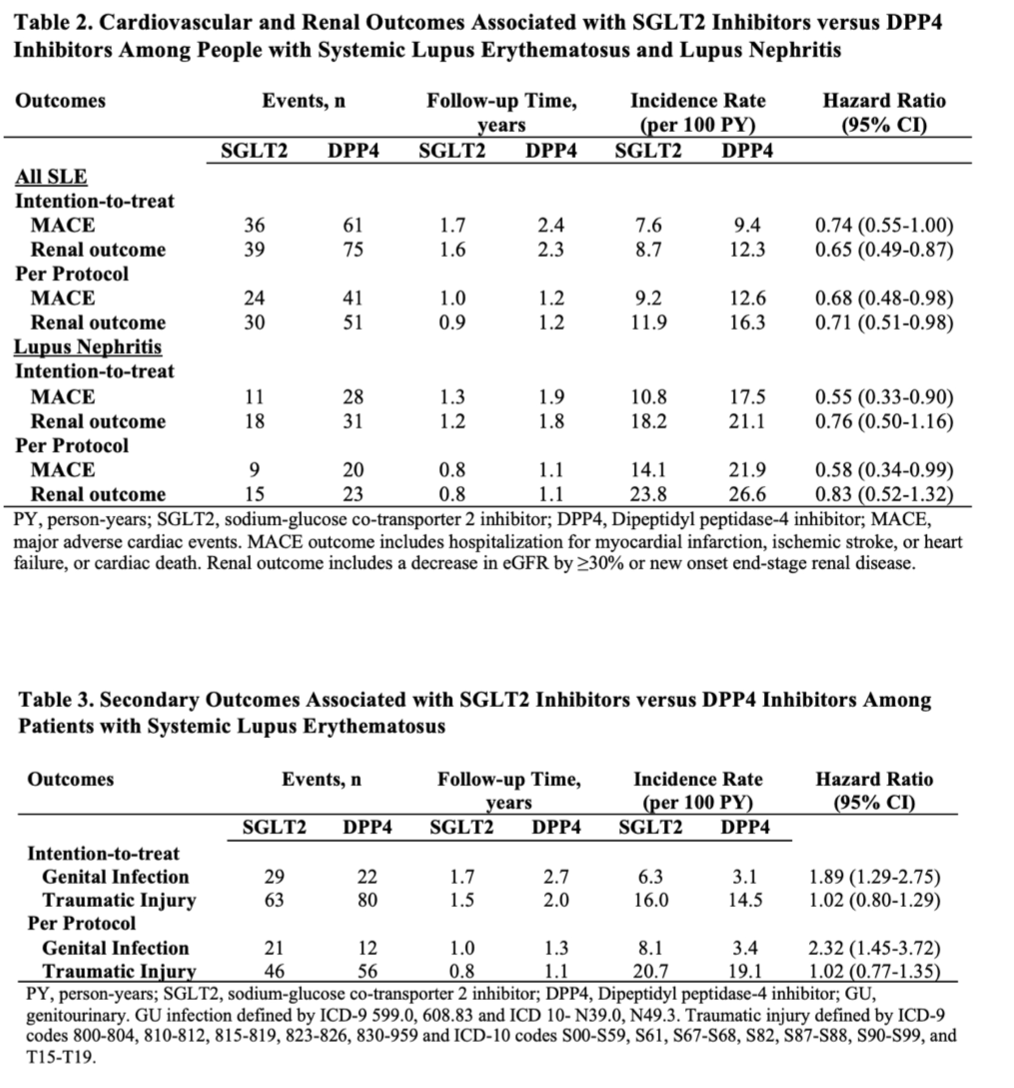
In their cohort, Dr. Jorge reports that SLE pts who used SGLT2i had⬇️risk of MACE(HR 0.69 [95% CI 0.48-0.99]) & renal progression(HR 0.71 [95% CI 0.51-0.98]) vs DPP4 use
Risk of MACE also⬇️in LN subgrp
🧐💊A potential role of SGLT2i for SLE/LN?
#ACR23 ABST1579 @RheumNow #ACRbest https://t.co/Dod8DqRvLo
sheila ( View Tweet )
2 years 7 months ago
#ACR23 @RheumNow
SGLT2 inhibitors help CV & renal outcomes, but SLE pts excluded @AprilJorgeMD
ComparedSGLT2 to DPP4 inhibs, real world observation emulation study in SLE pts with T2DM
Lower incidence of MACE & renal progression
Subgroup w LN - risk reduction 10.2 MACE/100 py https://t.co/JpJ0yWNQBe
Eric Dein ( View Tweet )
2 years 7 months ago
Excellent start to Plenary II
Should we borrow SGLT2i and DPP4i use from endocrine?
SLE pts who initiated SGLT2 or DPP4: lower risk of MACE and renal progression
@RheumNow #ACR23 Abs#1579 https://t.co/RsaWuetyft
Robert B Chao, MD ( View Tweet )
2 years 7 months ago
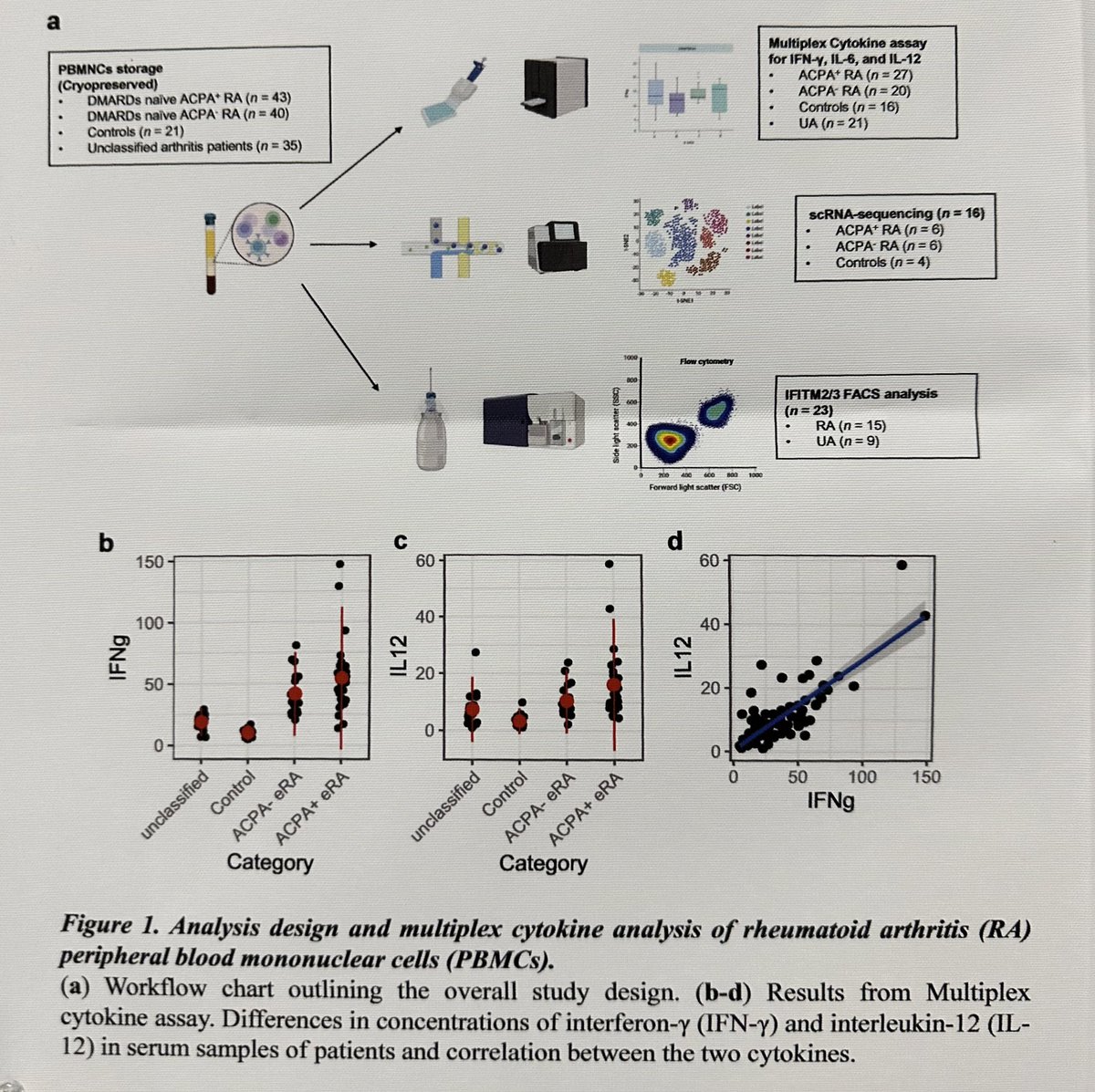
RA peripheral blood mononuclear cells display IFN-gamma signature
Driven by 2 cell subsets: T cells & macrophages
IFNg driven transcription factors
Increased only in ACPA+ RA
Differential biology could inform ACPA stratified therapy
ABST1271 @RheumNow #ACR23 https://t.co/EN2noKGupK
Aurelie Najm ( View Tweet )
2 years 7 months ago
Glucocorticoids-free zone in SLE?
For over 70 years, glucocorticoids, (GC) have been a part of standard therapy in SLE. They are classically used to not only induce remission or treat an acute flare, but also as maintenance therapy. #ACR23
https://t.co/sfRhNj6OpZ https://t.co/k6VoG5lKO7
Dr. John Cush @RheumNow ( View Tweet )
2 years 7 months ago

To remind us. Glory be! GLORIA a #RCT in elderly active #RA: MTX+10 mg daily #prednisolone which was better than MTX alone. But more infections and no comparison of inexpensive Rx such as adding #HCQ. Still debated as to benefit vs risk of this strategy @RheumNow #ACR23 @ACRheum https://t.co/slOmESbIOW
Janet Pope ( View Tweet )
2 years 7 months ago
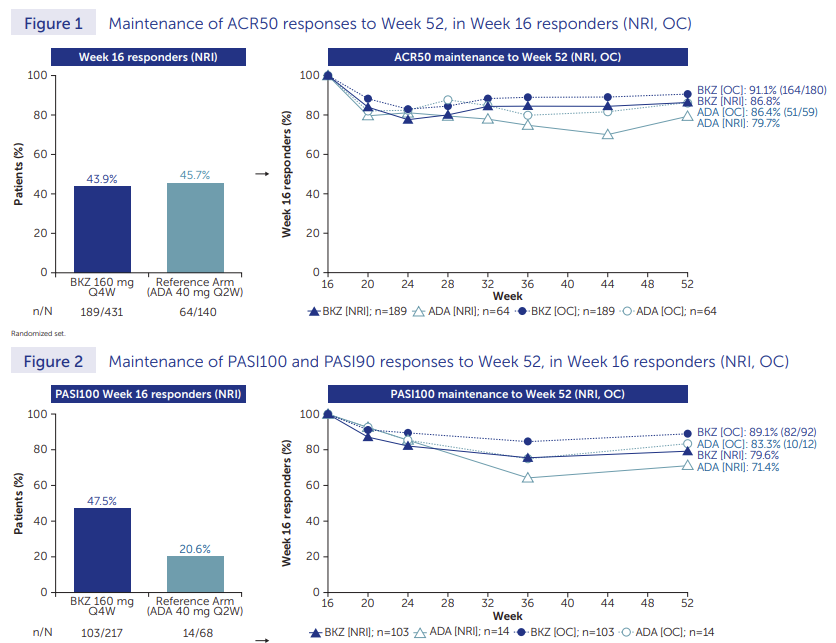
Rather unsurprising finding at this point, but valuable nonetheless
Per usual, joint efficacy for bimekizumab (IL17i) ~similar to TNF
New twist; similar loss in efficacy over time. Nice to have another IL17i; not sure this is a "blockbuster"
@RheumNow #ACR23 Abstr1437 https://t.co/4sVfSz7ZnK
Mike Putman @EBRheum ( View Tweet )
2 years 7 months ago
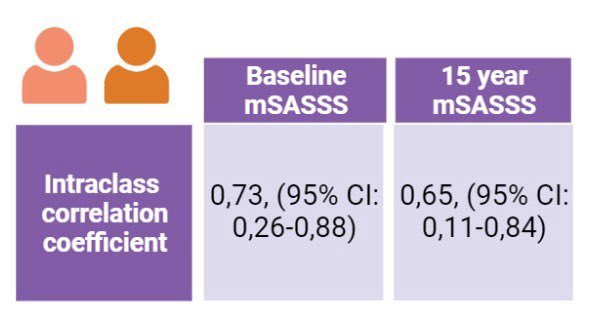
In axSpA, the mean and median progression were 0.54 and 0.38 points in mSASSS per year respectively, lower than what has been reported in similar cohorts, LBP before diagnosis was a strong predictor of progression, Granados R Abst#1389 #ACR23 @RheumNow https://t.co/fvkOzhUG97 https://t.co/k18HxWswbs
Dr. Antoni Chan ( View Tweet )
2 years 7 months ago
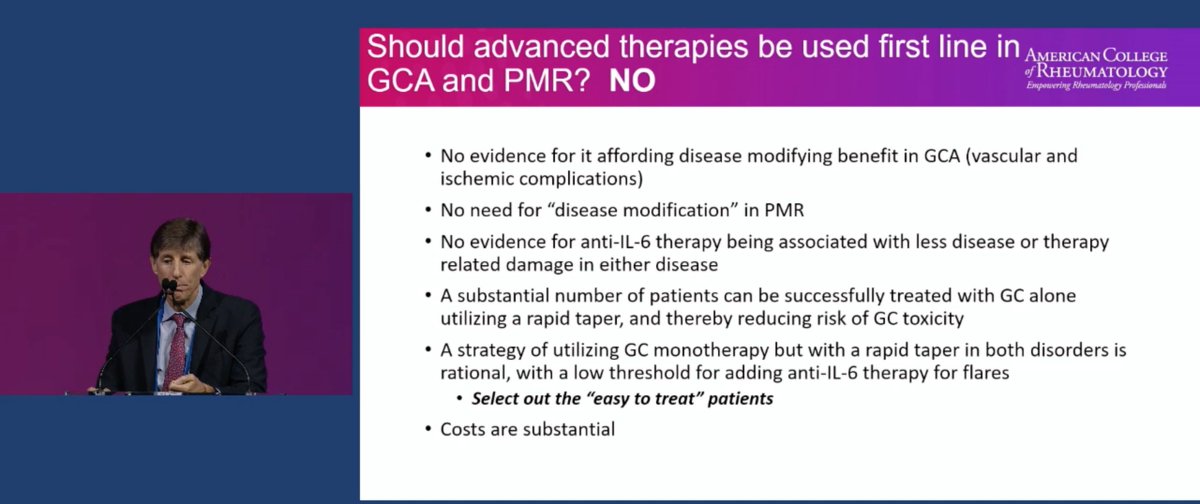
Great Debate on the use of biologics in treatment of Giant Cell Arteritis and Polymyalgia Rheumatica!
Let's begin with Dr. Robert Spiera on why we should NOT use IL-6i
No evidence of disease modifying
Lose biomarker activity
Cost
@RheumNow #ACR23 #ACRbest https://t.co/XCT02wYb2s
Robert B Chao, MD ( View Tweet )
2 years 7 months ago
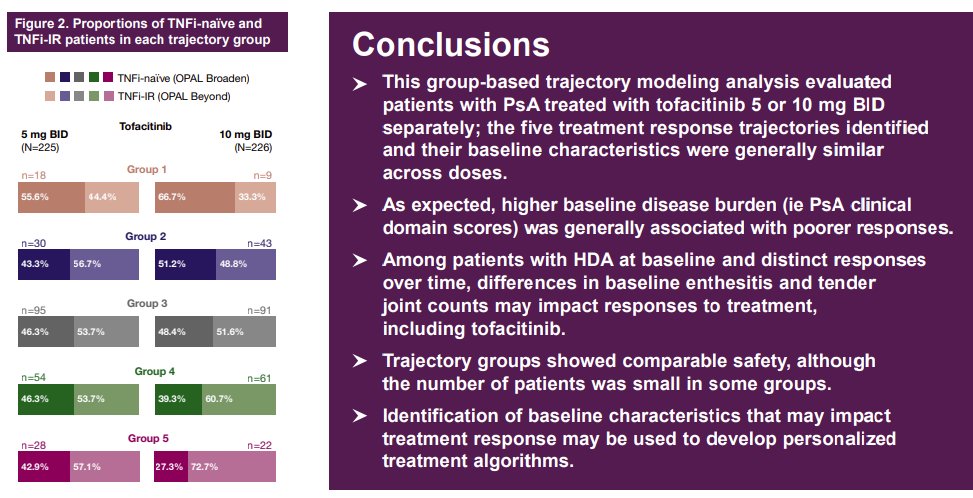
Interesting abstract re:dx trajectories, I have a counter-intuitive take
I expect pts w/high dx activity to respond BETTER than pts w/LDA at diagnosis
More autoimmunity + less fibro = higher chance to respond to DMARD?
Anyone else feel that way?
@RheumNow #ACR23 Abstr1426 https://t.co/D6GU7tMcY6
Mike Putman @EBRheum ( View Tweet )
2 years 7 months ago
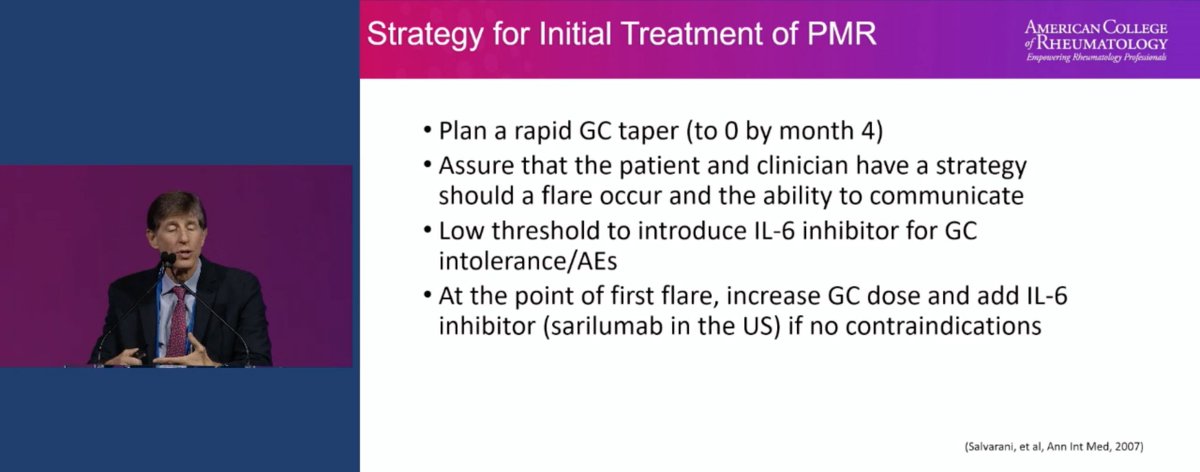
How does Dr. Robert Spiera manage GCA?
1) Tx with steroids alone, taper by 6 months
2) Do not chase ESR/CRP
3) Pay attention to steroid complications
4) Low threshold to use IL-6i
Similar plan for PMR
Taper steroids by month 4
@RheumNow #ACR23 https://t.co/KSwyfjobFY
Robert B Chao, MD ( View Tweet )
2 years 7 months ago
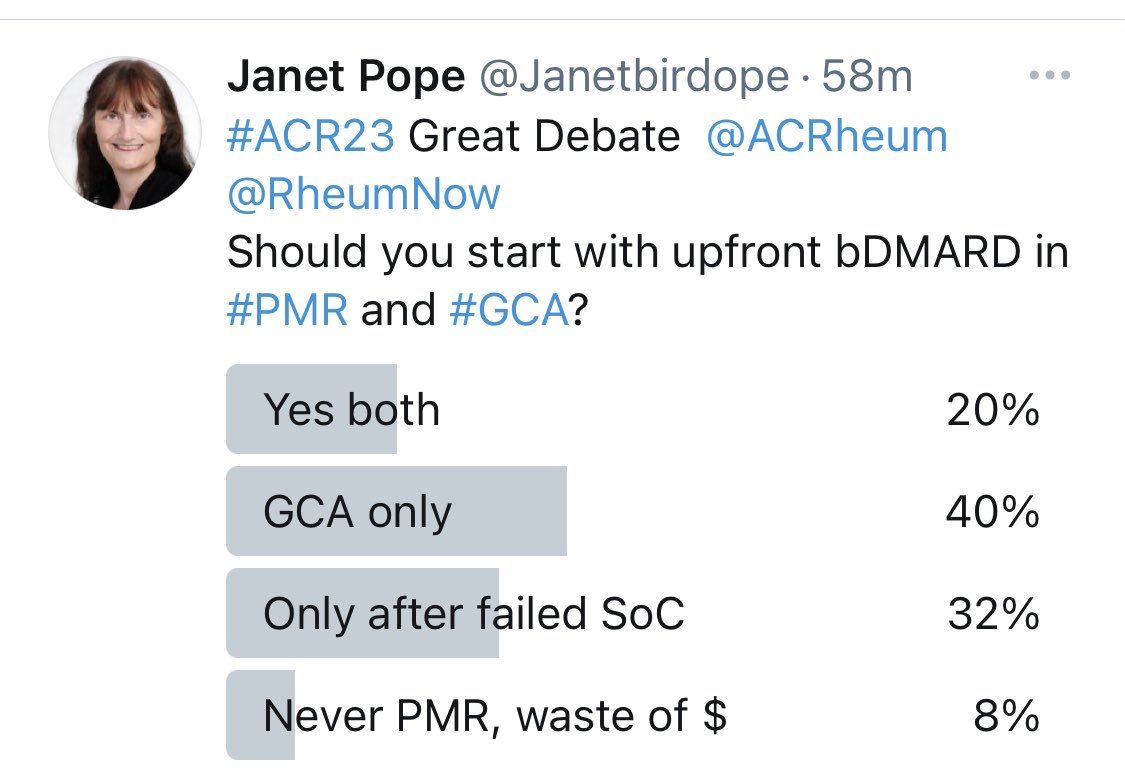
Here is the popular answer@to the #ACR23 debate of up front bDMARD in GCA and PMR Yes vs No. the audience has no consensus. Access is Impt, experience and criteria of who to use it in. @ACRheum @RheumNow https://t.co/7pxF4w926m
Janet Pope ( View Tweet )
2 years 7 months ago

