
All News

ACR23 – Day 3 Report
These year’s annual ACR Convergence has been a success with the return of an insanely active Poster Hall! F2F learning amidst miles of research and many young talented aside wizened establish presenters is such a welcome return to ACR, the way it should be.
Read Article
Less (Glucocorticoids) is More in Lupus Nephritis
Dr. Yuz Yusof talks with Dr. Amir Saxena about abstract 0781 at the 2023 ACR Convergence meeting in San Diego, CA.
https://t.co/EriaJvBPj9 https://t.co/x5hNIAgBz2
Dr. John Cush RheumNow ( View Tweet)
L16 @ #ACR23
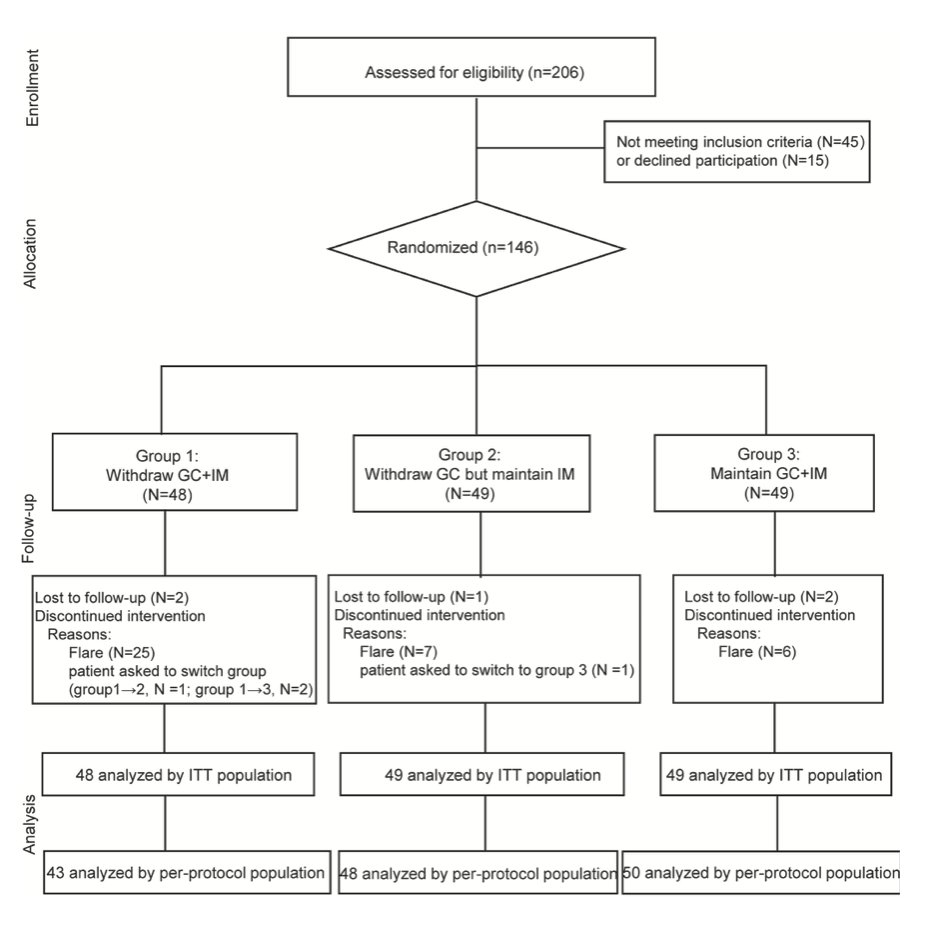
⭐️Can you discontinue glucocorticoids (GC) & immunosuppressive agent (IM) in stable IgG4-RD (clinically quiescent for at least 12 mo)?
➡️146 pts followed for 18 mo:
👉Group 1: withdraw GC+IM
vs
👉Group 2: withdraw GC… https://t.co/j77xYm9qSN https://t.co/72IwBeEwv9
Meral K. El Ramahi, MD MeralElRamahiMD ( View Tweet)
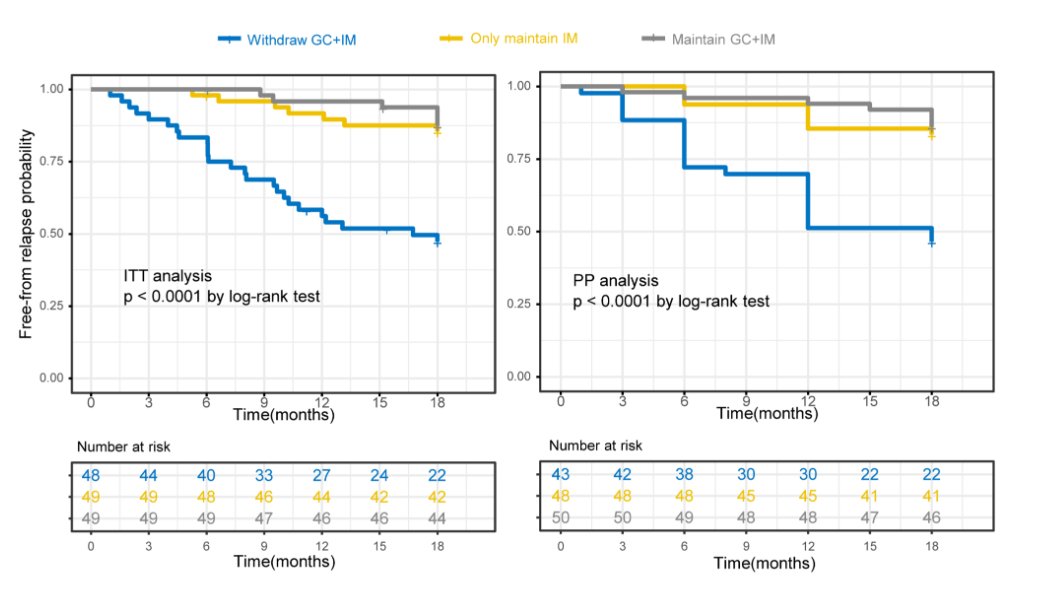
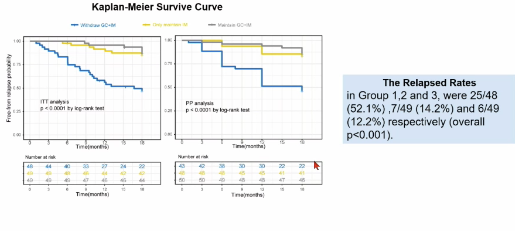
Peng et al. 146 IgG4-RD in remission on immunomodulators+GC. 18 month follow-up. Withdraw IM+GC - 52% flare. Withdraw GC + continue IM 14.2% flare. Continue both 12.2% flare. Clear message that ongoing IM is the way Abstr#L16 #ACR23 #ACRbest @RheumNow https://t.co/3CAQhyTYqq https://t.co/qr1GOSvJYg
Richard Conway ( View Tweet)
L16 #ACR23 @RheumNow
W/d of Immunosuppr and Low-dose steroid in IgG4RD
Gr1: W/d GC+IM, G2: IM alone, G3: Maintain
Relapse rate: G1 52%, G2 14%, G3 12% https://t.co/xe6NLVxUov
Eric Dein ( View Tweet)
Withdrawing immunosuppression and steroids in IgG4-RD
Maintaining immunosuppression with or without steroids associated with low relapse rate
52% of pts who withdrew steroids +immunosuppression relapsed
@RheumNow #ACR23 Abs#L16 https://t.co/xJyDiCkMVD
Robert B Chao, MD ( View Tweet)

Withdrawal of Immunosuppressant and Low-dose Steroids in IgG4-RD Patients with Stable Disease
146 pts - 3 Grps
1: withdraw GC+IM 2:withdraw GC but maintain IM; 3: maintain GC+IM
The maintenance of IMs, with or without low-dose GC, superior to withdraw
#ACR23 @rheumnow #abstL16
Bella Mehta bella_mehta ( View Tweet)
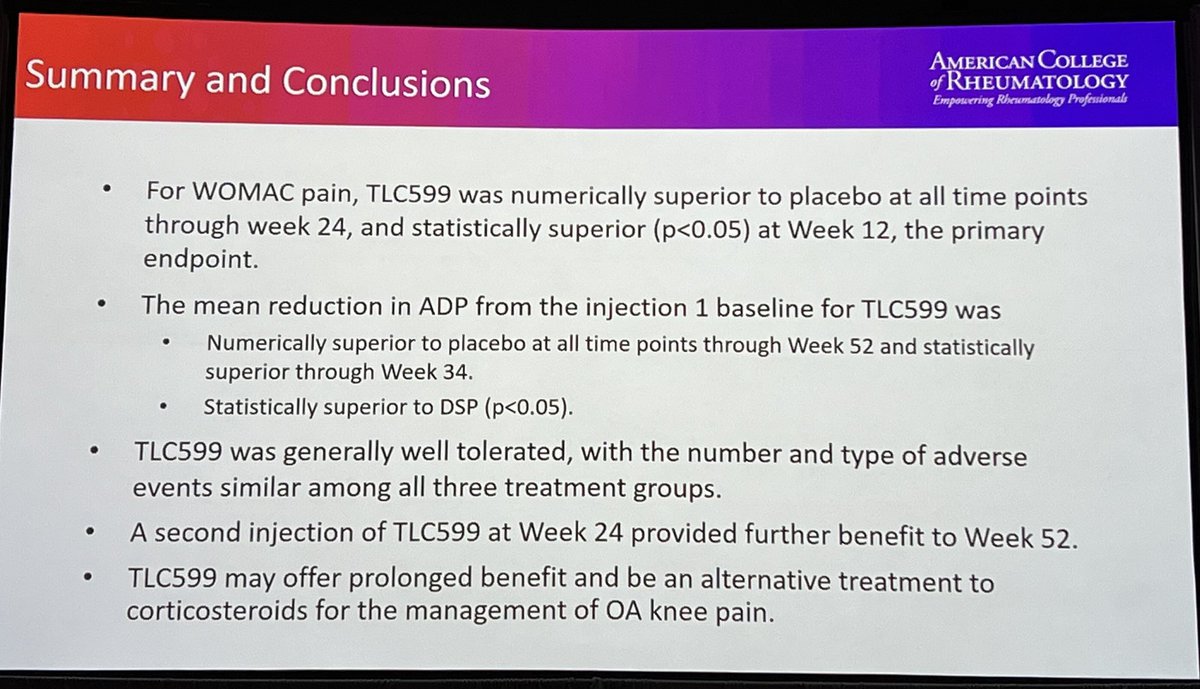
#ACR23 Late-Breaking Abstr#L19 IA steroid can help osteoarthritis knee pain but effect & duration are variable. Phase 3 RCT: improvement in ADP & WOMAC pain favouring TLC5999 (liposomal modification of DEX) vs PBO at all timepoints inc. after repeated injection @RheumNow #ACRBest https://t.co/xUhoFHPExr
Md Yuzaiful Md Yusof ( View Tweet)
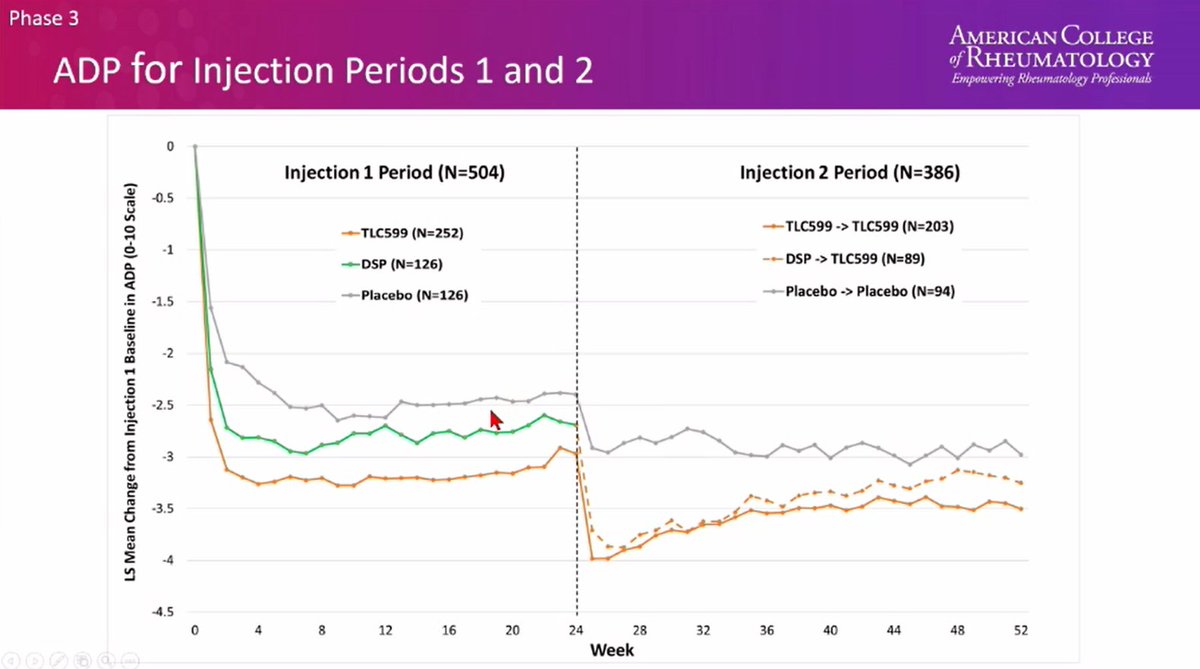
Would intraarticular steroids for knee OA be better with a sustained release formulation?
ph3, TLL599 (liposomal delivery dexamethasone) vs normal dex vs placebo
some gains over normal dex
well tolerated
New options always welcome in OA!
@ProfDavidHunter #ACR23 L19 @RheumNow https://t.co/TUrhppHMiD
David Liew drdavidliew ( View Tweet)

What happens when you stop #steroids and/ immunosuppressive Rx in Pts in remission for at least 1 yr in #IgG4 disease?
You are likely guessing correctly
Pts flare! Don’t stop Rx
?taper 🤷♀️
Like RA Rx - if stop Rx = flares
Large RCT from China L16 #ACR23 @RheumNow @RheumNow
Janet Pope ( View Tweet)
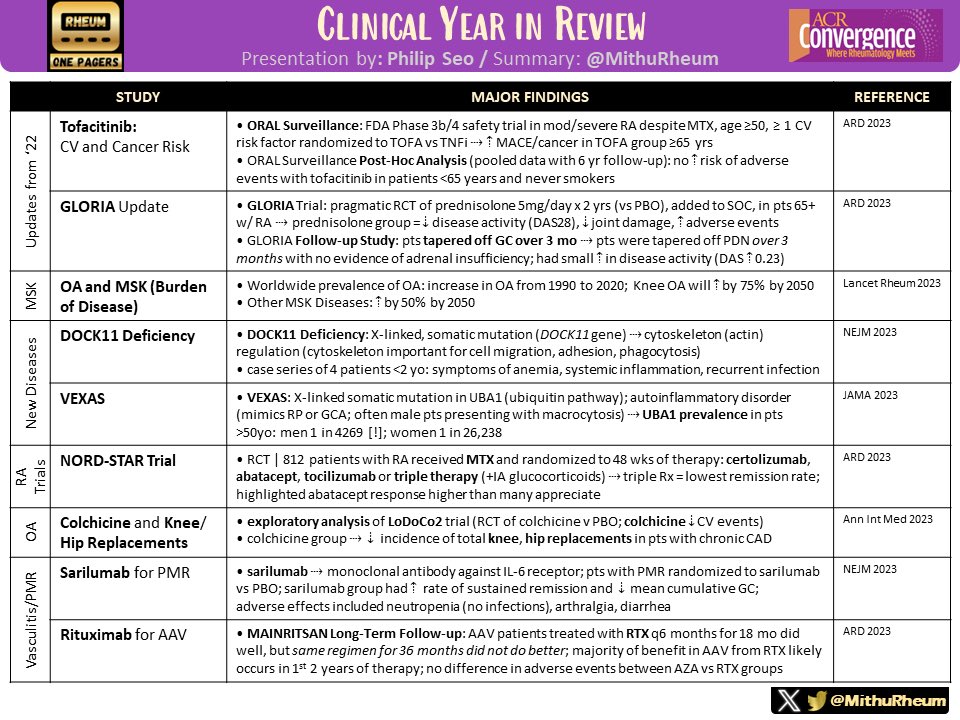
Clinical Year in Review at #ACR23
By @philseo (@jhrheumatology)
Review some of the most impactful scientific studies in #Rheumatology in the past year! 🍕 https://t.co/ystEjzrU8u
Mithu Maheswaranathan, MD ( View Tweet)
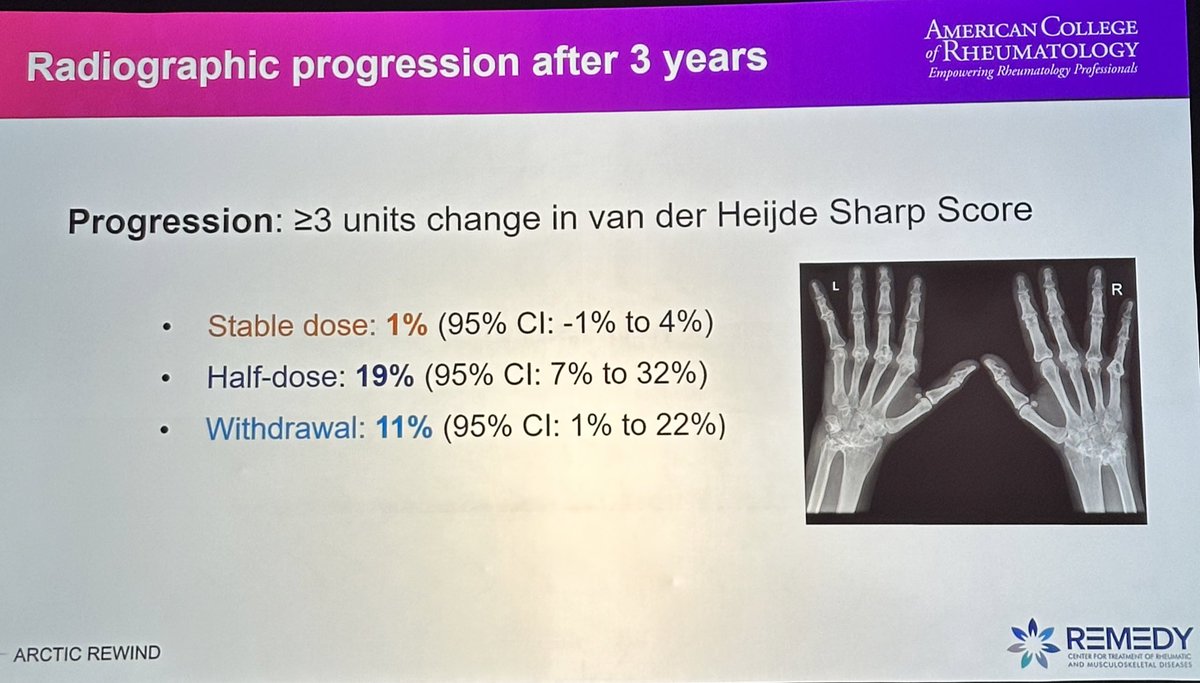
ARTIC REWIND RCT 3 yrs csDMARD withdrawal
38% 3yrs csDMARDs free remission vs. 80% stable dose gpe
75% recovery after restart
Rx progression 19% in half dose gpe
More use bioDMARDs (18%) & GCs (50%) withdraw gpe
Trends towards lower infections
@RheumNow #ACR23 #ACRBest https://t.co/jhOINV7LLS
Aurelie Najm ( View Tweet)
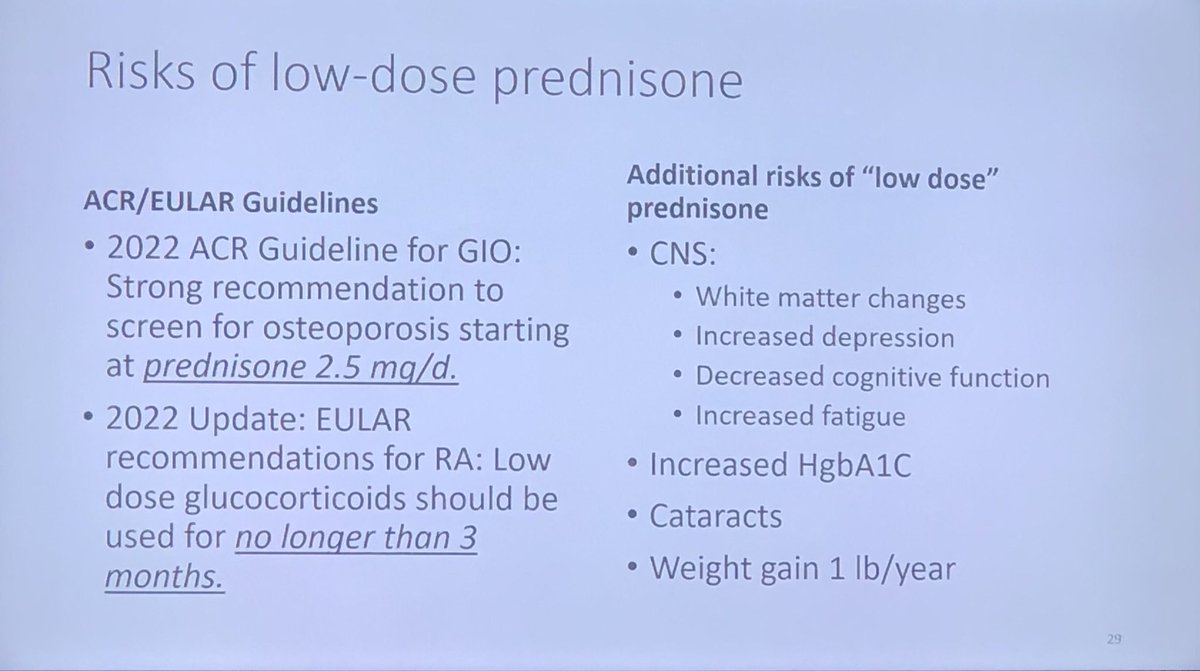
Low dose #prednisone has (bad) brain effects. An argument to use steroid sparing drugs in #PMR @philseo @ACRheum @RheumNow #ACR23 THINK about steroid sparing Rx in ?all pts with #PMR #Great #debate https://t.co/usQJRNUN8B
Janet Pope ( View Tweet)
Rx of #inflammatory #arthritis with #glucocorticoids doesn’t seem to affect outcomes in #malignancy treated with #checkpoint #inhibitors. Good news as new or flaring inflammatory arthritis as an irAE can be severe. #ACR23 @RheumNow @ACRheum #1055 @CanRIO_Tweets https://t.co/tFIPcQq2X6
Janet Pope ( View Tweet)
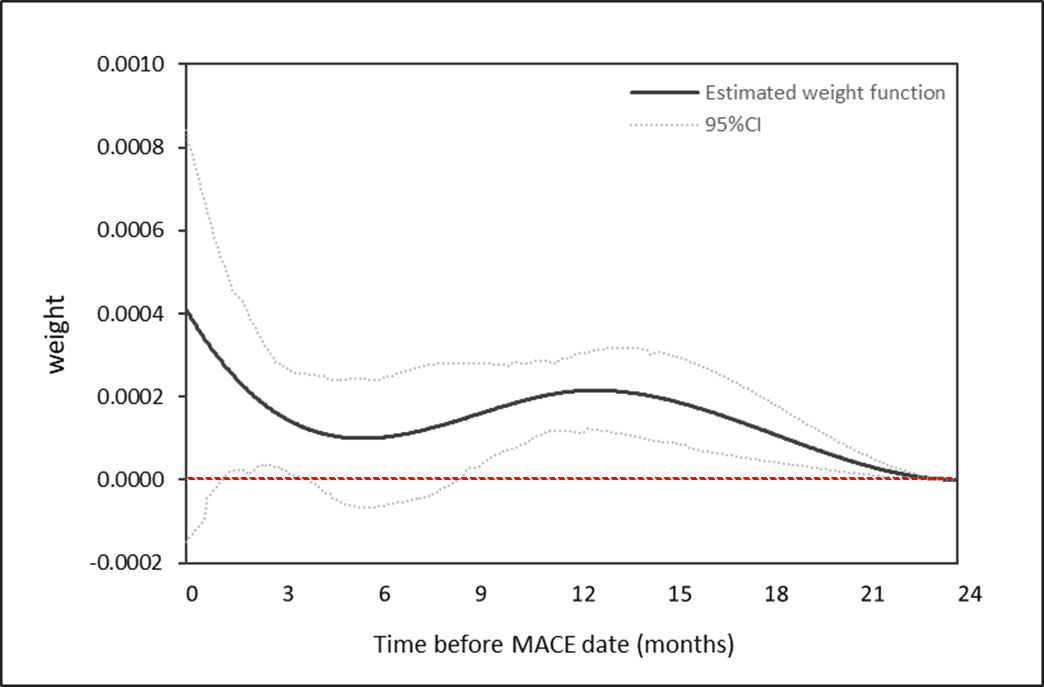
There is a dose, duration and recency-dependent relationship between previous GC use and MACE. GC doses 5mg/day, durations of 30 days, and use one year prior to MACE were all associated with an increased risk of MACE, Wallace B Abst#2430 #ACR23 #ACRBest https://t.co/2ExboBvo2W https://t.co/FuqXdFFwqP
Dr. Antoni Chan ( View Tweet)
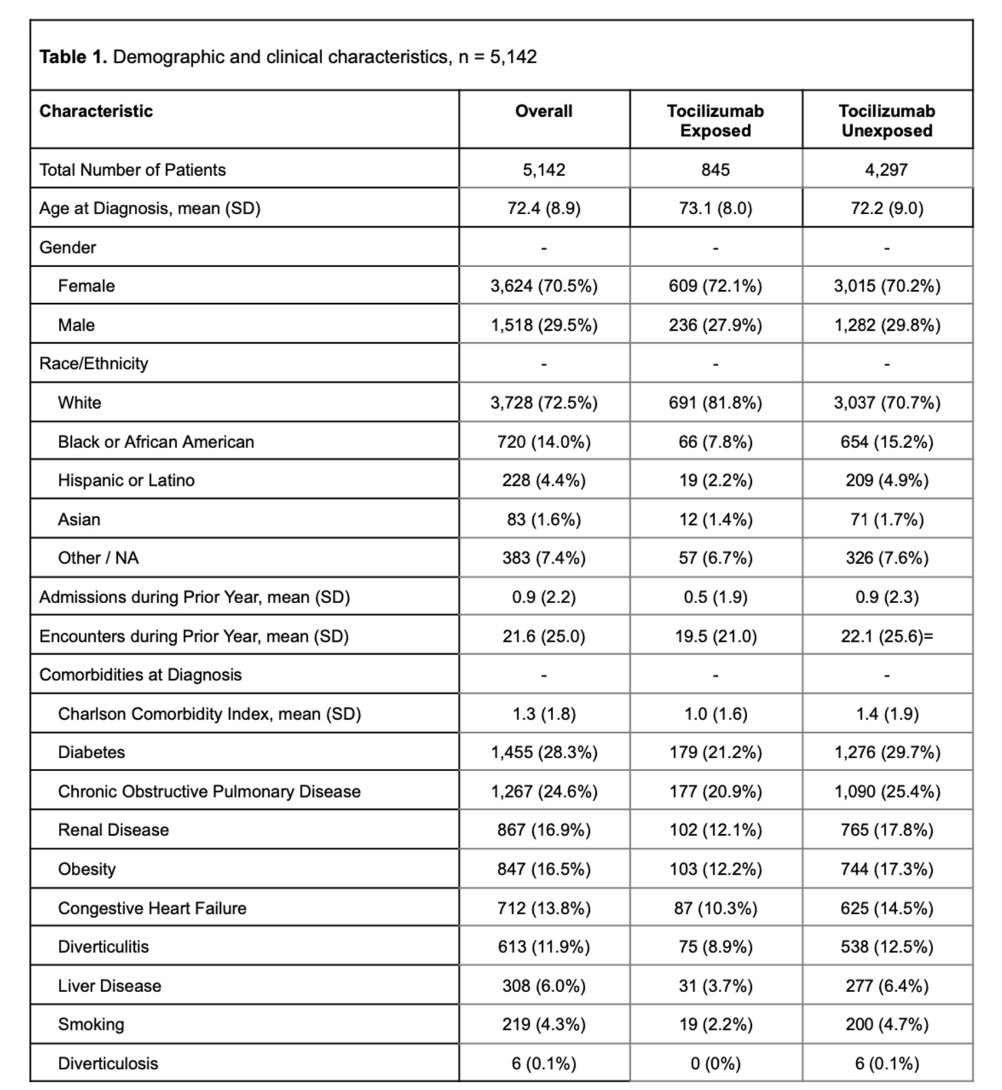
Nepal et al. No increased risk of GI perforation for tocilizumab in GCA HR 1.05 . Diverticulitis (RR 3.51), IV methylprednisolone (RR 5.41) risk factors. This fits with my priors, steroids are a bigger risk than tocilizumab. Abstr#2560 #ACR23 @RheumNow https://t.co/BAmBQA0kEP https://t.co/zRjmDIkOHp
Richard Conway ( View Tweet)
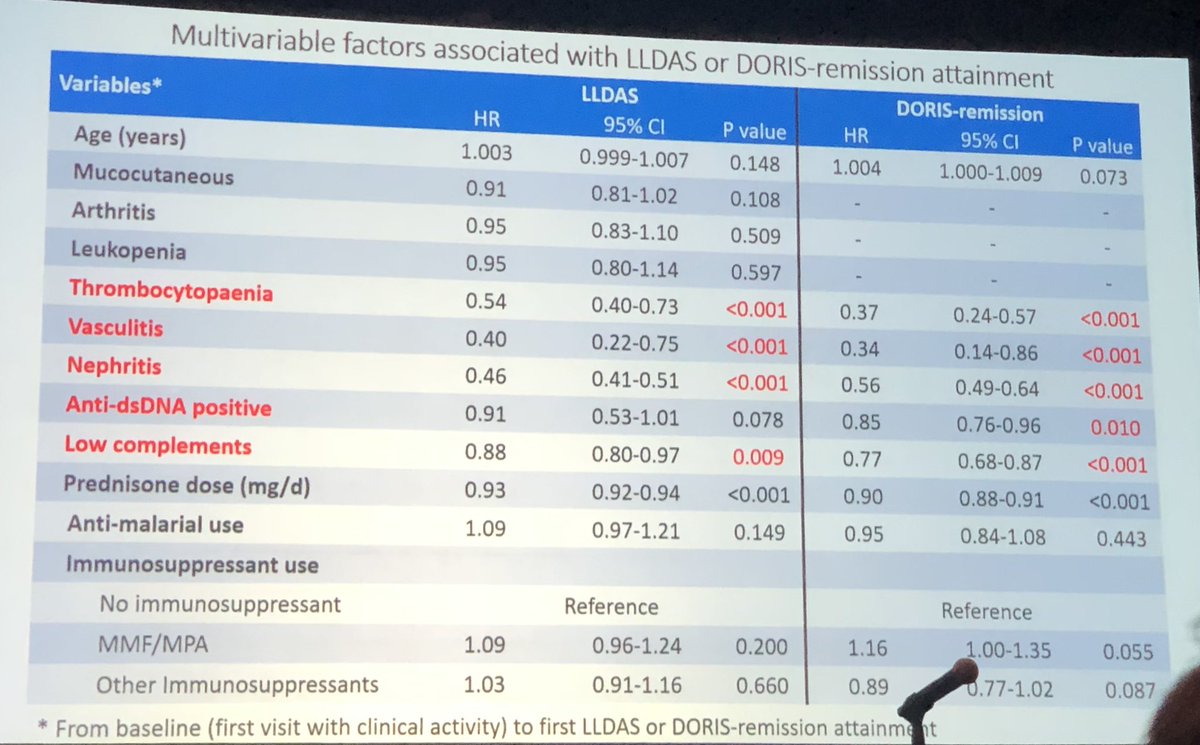
After attaining #remission or #LLDAS after a flare - HALF flare over f/u esp if tapering pred to <7.5 or 5 mg. #HCQ was protective. 65% got LLDAs and 45% rem in 1/2 yr - longer time to get #remission #2553 #ACR23 @RheumNow @ACRheum #ACRbest Asian cohort of #SLE largest@in world https://t.co/yBBqYJZVOe
Janet Pope ( View Tweet)

Fantastic presentation by Desh Nepal from MCW on risk of GI perforation in patients with #GCA
Low incidence , no association with TCZ, but increased risk with IV methylprednisolone and h/o diverticulitis.
@EBRheum #ACR23 https://t.co/bgvmjAXBEY
Sebastian E. Sattui MD, MS SattuiSEMD ( View Tweet)

GCs on MACE in RA in VA
A#2430 #ACR23 @RheumNow
Not just ongoing steroid usage, also prior usage 1 year ago
5 mg use for 30 days one year ago - increases MACE events by 3%
5 mg use for 90 days one year ago - increases MACE events by 9%
Eric Dein ( View Tweet)
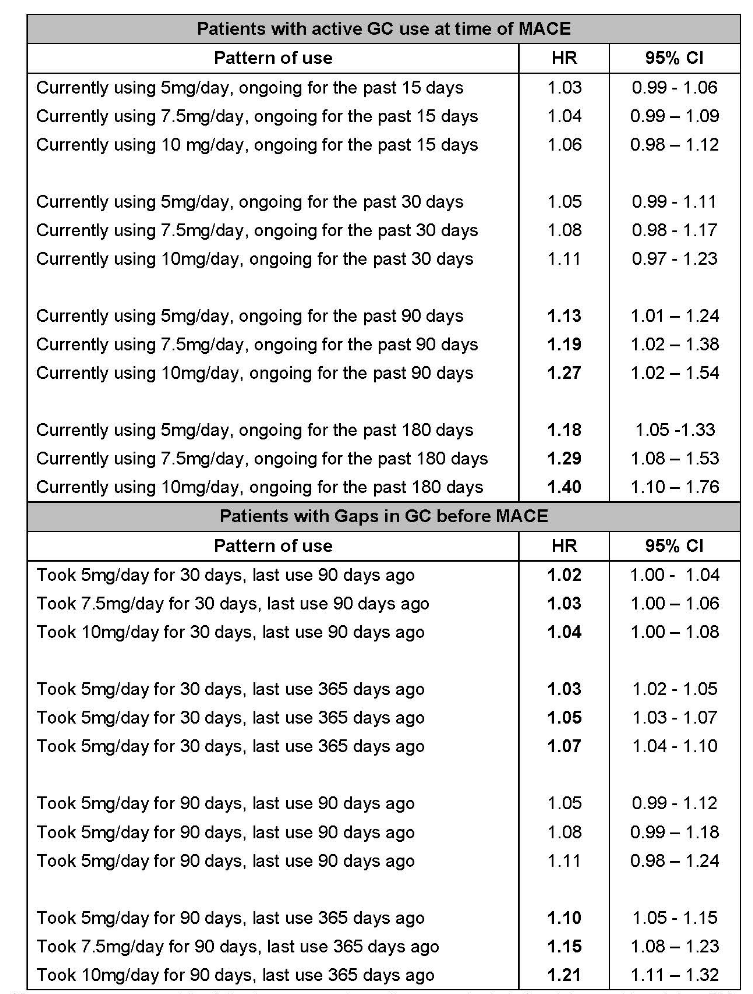
Wallace et al. Dose, duration, recency dependent relationship between GC and MACE. Even 5mg/day, 30 day use, and use 1 year prior associated with risk. 5mg, 7.5mg, 10mg pred for 90 days - 13%, 19%, 27% MACE increase Abstr#2430 #ACR23 #ACRbest @RheumNow https://t.co/50B5nGqxu9 https://t.co/lNrUbZOm0o
Richard Conway ( View Tweet)

