
All News

What’s New PsA? (4.3.2026)
Dr. Jack Cush reviews the news and major articles from this week, including FDA safety warnings, reports from AAD, PsA trials.
Read Article
Update on Primary CNS Angiitis
The Journal of Neurology has posted a review and update of Primary CNS vasculitis (PCNSV), also termed primary angiitis of the CNS (PACNS). PCNSV is rare, potentially fatal, and highly treatable, making timely recognition and accurate diagnosis critical.
Read Article
"When there are conflicting diagnostic possibilities, trust your excellent history and physical examination more than laboratory testing and imaging."
- Arthur Weinstein, MD
Dr. John Cush RheumNow ( View Tweet)

FDA has issued a drug safety warning for avacopan (Tavneos), dentifying 76 cases of drug-induced liver injury, including 7 cases of rare vanishing bile duct syndrome (VBDS). There were 8 deaths https://t.co/2GkYNg1Apn https://t.co/fW2qafKCew
Dr. John Cush RheumNow ( View Tweet)
Myocarditis causes 17,000 deaths/Yr worldwide. Causes include A) iatrogenic/autoimmune: checkpoint inhibitors & gene therapy; B) High income countries: parvo B19, herpesvirus 6; C) low income: dengue, HIV, malaria and Trypanosoma cruzi (Chagas disease) https://t.co/0FjPyXygpz https://t.co/04J23AiqtK
Dr. John Cush RheumNow ( View Tweet)
Target trial emulation: biologics or JAK vs RTX in RA-ILD -- abatacept (n=694), JAKi (156), IL-6i (389), or TNFi (734), PS-matched =# RTX; no significant differences (HR 0.74-1.09 NS) in outcomes of resp hosp, lung transplant & death. But ABA (HR 0.84) & JAKi (HR 0.62) had less https://t.co/c9IVwQYwMN
Dr. John Cush RheumNow ( View Tweet)

What's it like to have RA? LISA: "It only took me three short years to go from rock climbing to a power wheel chair and that stage of the disease was frightening and painful and you feel hopeless and as if your life plan is being stolen from you. Once I was able to start https://t.co/d49htc8k4m
Dr. John Cush RheumNow ( View Tweet)

Large pharmaceutical companies reduced their workforces by more than 22,000 employees in 2025. Among 17 largest companies , only five logged a head count increase in 2025 https://t.co/VdtlUaF4Q3 https://t.co/2xsCs9O1Tw
Dr. John Cush RheumNow ( View Tweet)
Retrospective study of 1st SLE pregnancies from LUNA Registry. Fetal loss was associated w/ aPL (OR 2.46) & pulse steroids (2.46), but not w/ SSA Abs (1.32). 247 pregs, 194 live births, 53 fetal loss. Ro+ vs Ro- no difference in live births or preterm births https://t.co/bsMMvVyffw
Dr. John Cush RheumNow ( View Tweet)

What's it like to have #RA? RICHARD: "There were days that I couldn’t mask the pain or hide the limp..So I tried to deny and hide the disease. I would always go up and down stairs when no one was looking. I got up extra early so no one could see me walk like an old man to the https://t.co/krHn4yoRYd
Dr. John Cush RheumNow ( View Tweet)
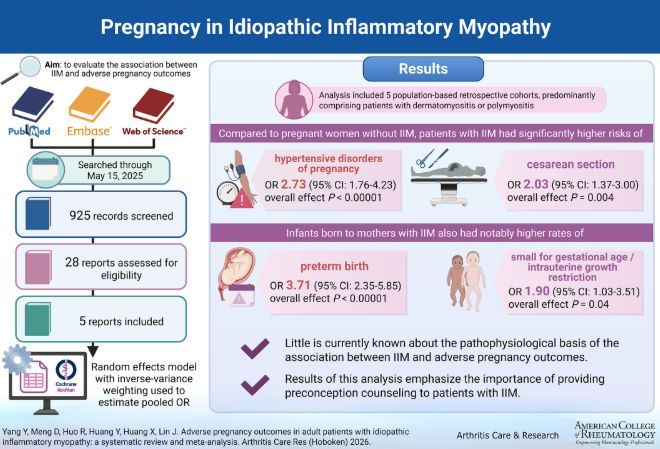
5 Retrospective cohorts of PM/DM pts showed IIM (myositis) had signif higher risks of IIM patients HTN w/ pregnancy (OR 2.73), & C-section (OR 2.03). Also more preterm birth (3.7), SGA/IUGR (1.9) https://t.co/w6qymR0I2w https://t.co/ovtwdleRfE
Dr. John Cush RheumNow ( View Tweet)

A new review of the GLP-1 receptor drugs @NEJM
https://t.co/PK03jApZWB
surprisingly, the word inflammation only appears once, in this diagram https://t.co/1PeBakBAQb
Eric Topol EricTopol ( View Tweet)

Advanced Practice Rheum: Rheumatoid & Inflammation Testing
In this review, we'll be talking about labs, inflammation, and tests for rheumatoid arthritis.
https://t.co/UbEoBz37hT https://t.co/V9WzfRtbFQ
Dr. John Cush RheumNow ( View Tweet)

Ixekizumab With Tirzepatide Efficacy in Obese Psoriatic Arthritis
The TOGETHER-PsA trial has demonstrated the efficacy and safety of ixekizumab (IXE) administered with tirzepatide (TZP) in adult active psoriatic arthritis (PsA) patients who were overweight or obese. https://t.co/KFwfi9FaAh
Dr. John Cush RheumNow ( View Tweet)
AAD 2026 Annual Mtg presents new data on another TYK2 inhibitor. In 2 phase 3 RCTs (ONWARD1 ONWARD2) envudeucitinib was superior to placebo & apremilast in 1700 plaque psoriasis pts https://t.co/DPlzDw5m7N
Dr. John Cush RheumNow ( View Tweet)

What's it like to have #RA? PATTY "To find patients or doctors who can talk intelligently about RA is a welcomed relief. However, I prefer that those around me not know about me and my RA. I hope they don’t notice the changes in my hands or shoes or that I cannot wear my usual https://t.co/OQbXJrcyPp
Dr. John Cush RheumNow ( View Tweet)

After hours EHR catchup has been coined "Pajama time" by residents & physicians & contributes to burnout. Survey 9,731 YR 2 Family Med residents- spend 3+ hrs/d after wk on ambulatory EHRs. Pajama time assoc w/ less knowledge, professional satisfaction, more burnout. https://t.co/QSR7VM2T7u
Dr. John Cush RheumNow ( View Tweet)

Brepocitinib in Dermatomyositis
The NEJM reports that brepocitinib, an oral TYK2–JAK1 inhibitor, was studied in a phase 3 trial of refractory dermatomyositis (DM) patients and shown to have significant benefits at the higher dose.
https://t.co/YNxrVTIubb https://t.co/uFY3kMOvui
Dr. John Cush RheumNow ( View Tweet)

AFFINITY Study - Combination Biologic Therapy in PsA
A pilot trial assessed the efficacy and safety of the guselkumab+golimumab (COMBO) combination versus GUS monotherapy in active PsA (failing a prior tumor necrosis factor inhibitor (TNFi-IR) and showed superiority in ACR 50 https://t.co/f2CB8FnZMB
Dr. John Cush RheumNow ( View Tweet)

FDA has issued a drug safety warning for avacopan (Tavneos), dentifying 76 cases of drug-induced liver injury, including 7 cases of rare vanishing bile duct syndrome (VBDS). There were 8 deaths https://t.co/WkBhs1rNpf https://t.co/ZXdHsAJUOQ
Dr. John Cush RheumNow ( View Tweet)

