

Update on Primary CNS Angiitis Save

The Journal of Neurology has posted a review and update of Primary CNS vasculitis (PCNSV), also termed primary angiitis of the CNS (PACNS). PCNSV is rare, potentially fatal, and highly treatable, making timely recognition and accurate diagnosis critical.
PCNSV is characterized by inflammatory destruction of CNS vessel walls, causing occlusion and infarction, with three histopathologic subtypes: granulomatous, lymphocytic, and necrotizing. PCNSV is isolated to the CNS with little or no systemic inflammation — distinguishing it from secondary CNS involvement in systemic vasculitides such as microscopic polyangiitis or rheumatoid vasculitis.
PCNSV has no pathognomonic clinical presentation and can be acute, subacute, chronic, or relapsing-remitting. Common features include headache, encephalopathy, cognitive decline, seizures, and focal neurological deficits. Three recognizable phenotypes should raise clinical suspicion:
- Acute/subacute encephalopathy, that may progress to coma.
- An MS-like relapsing-remitting picture — with seizures, severe headaches, encephalopathic or stroke-like episodes, and sometimes optic neuropathy; atypical features should prompt vasculitis consideration.
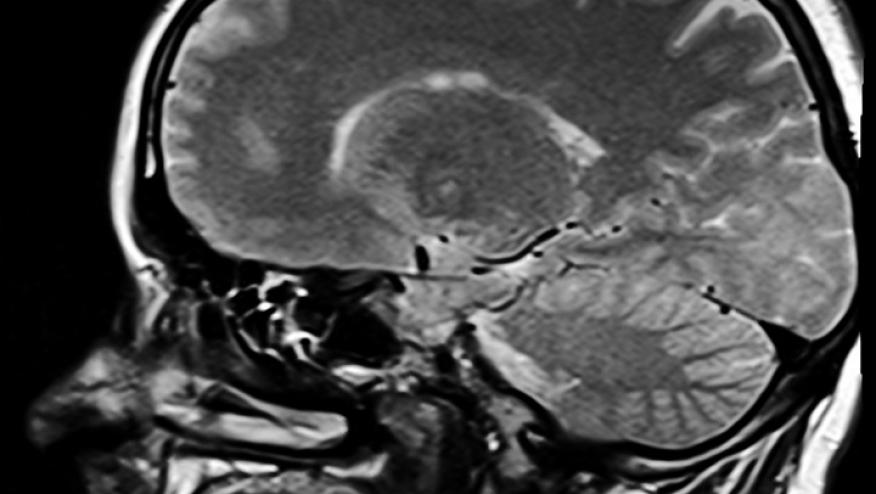
- Intracranial mass lesion(s) with headache, drowsiness, focal signs, and raised intracranial pressure. These may be mistaken for CNS neoplasm.
Mild systemic features (low-grade fever, night sweats, oligoarthropathy) may be present and should not be used to exclude PCNSV. Unilateral disease, while unusual, is well documented.
Diagnosis
No single blood, CSF, or imaging test is diagnostic. Workup serves primarily to exclude mimics — infection, malignancy, other CTD, reversible cerebral vasoconstriction syndrome (RCVS), atherosclerosis, drug-induced vasculopathy.
While the CSF is abnormal in approximately 75% of cases, and brain MRI in over 90%; but neither abnormalities are unique to PCNSV. In patients under evaluation you should consider: CBC, inflammatory markers, plasma viscosity (normochromic anaemia and neutrophilia are common), autoimmune serology, CT of chest/abdomen/pelvis, slit-lamp ophthalmoscopy, fundus fluorescein angiography, or whole-body CT-PET.
Distinctive findings may include:
- Cerebral Angiography: Multifocal segmental narrowing with beading is the classical vasculitic pattern, and digital subtraction angiography (DSA) remains the most sensitive and specific modality. However, sensitivity and specificity of catheter angiography are each only 25–35%, meaning a patient with 'typical' vasculitic changes is statistically more likely to have an alternative diagnosis. A normal angiogram does not exclude PCNSV.
- Vessel Wall MRI: High-resolution vessel wall imaging is advancing but has not yet been validated against neuropathology. Features such as vessel calibre abnormalities, ischaemic lesions of varying age, non-territorial distribution, and intramural gadolinium enhancement can inform interpretation — but rigorous MR-pathological correlation studies are still needed.
Brain Biopsy is considerted the "Gold Standard" and is the primary source of a definitive diagnosis. Sensitivity is 50–70%, but approximately 75% of patients receive a clinically actionable result (either confirmed PCNSV or a specific alternative diagnosis such as lymphoma or infection). Procedure-related mortality in multiple series is effectively zero. The risks of biopsy must be weighed against the dangers of misdiagnosis and empirical immunosuppression — particularly when the alternative is an occult infection or cerebral lymphoma. Biopsy has also revealed distinct PCNSV subtypes: Abeta-related angiitis (ABRA), small vessel inclusion body vasculitis (primarily paediatric), and hypereosinophilic CNS vasculitis — each with distinct prognostic and therapeutic implications.
The authors propose a binary classification replacing the traditional 'possible/probable/definite' framework:
- Definite PCNSV: Histopathological confirmation of CNS vasculitis plus exclusion of systemic vasculitis or secondary causes.
- Possible PCNSV: Clinical and investigative features consistent with PCNSV but without biopsy proof.
Treatment
No RCTs exist for PCNSV. All recommendations derive from expert consensus and extrapolation from systemic vasculitis trials (ANCA-associated, renal vasculitis).
Induction Therapy:
- High-dose corticosteroids combined with cyclophosphamide remain the standard of care for induction.
- Emerging data from systemic vasculitis trials suggest that combining rituximab with cyclophosphamide may safely reduce cumulative corticosteroid exposure — a strategy of potential relevance to PCNSV.
Maintenance Therapy:
- Azathioprine or methotrexate are preferred over mycophenolate mofetil for remission maintenance, based on systemic vasculitis RCT data (IMPROVE trial).
- Rituximab monotherapy has case-series support in PCNSV but nearly all reports lack histopathological confirmation, limiting interpretation.
Given the toxicity profile of induction agents and the life-altering consequences of misdiagnosis, histological confirmation before initiating aggressive immunosuppression is strongly recommended wherever feasible.
KEY TAKEAWAYS
- PCNSV is rare, potentially fatal, and highly treatable — diagnostic obscurity and therapeutic urgency makes this a challenging condition.
- There is no pathognomonic presentation. Three clinical phenotypes — acute encephalopathy, MS-mimic, and intracranial mass lesion — should prompt PCNSV consideration when other explanations are lacking.
- Cerebral angiography has a positive predictive value below 30% for PCNSV. 'Typical' vasculitic changes on angiography statistically more often represent an alternative diagnosis. A normal angiogram does not exclude disease.
- Brain biopsy is the diagnostic gold standard. It carries near-zero procedural mortality and yields clinically actionable results in ~75% of cases — including occult infections and cerebral lymphoma that would be harmed by empirical immunosuppression.
- Induction with high-dose corticosteroids plus cyclophosphamide remains standard; azathioprine or MTX is preferred for maintenance. Future progress depends on international, biopsy-proven cohort studies and collaborative clinical trials.
Continue Reading
Join The Discussion
Great narrative review by one of the leaders in the filed!
Kudos
Len Calabrese
Disclosures
The author has no conflicts of interest to disclose related to this subject
The author used AI to research and organize this content, and maintains responsibility for its accuracy






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.