

Evolution of GCA Treatments - More to Come Save


The field of Rheumatology is an ever-nascent field with an incredible expansion in our therapeutic armamentarium over the past half century. An example of such advancement is easily appreciated when reflecting on the innovative treatment approach to Giant Cell Arteritis (GCA), the most common form of vasculitis in patients older than 50 years of age.
What we have come to identify now as GCA was first described in 940-1010 AD in the following passage in the “Memorandum of Oculists” by Ali Ibn Isa:
“By these means one treats not only migraine and headache… but also acute, sharpy, catarrhal affections, including those showing heat in and inflammation of the temporal muscles. These diseased conditions may terminate in loss of eye sight.”
GCA was, again, described in 1890 as “thrombotic arteritis of the aged” and in 1932 as a systemic constitutional syndrome with temporal and scalp tenderness, but treatment with glucocorticoids (GC) was not described until 1949.
Through the combination of clinical experience and advancements in our diagnostic tool set, we now understand that GCA is a complex clinical syndrome with a heterogeneity in presentation that can include the following manifestations:
- Non-specific symptoms such as fever, night sweats, weight loss, fatigue, malaise, unexplained anemia, or dry cough
- Large vessel manifestations such as claudication, digital ischemia, asymmetric pulses/blood pressures, or arterial bruits
- Cranial manifestations such as headache, blurred vision, visual loss, jaw/tongue claudication, or temporal/scalp tenderness.
- Visual symptoms (amaurosis fugax or diplopia) without systemic manifestations dubbed accordingly as occult (silent) GCA. Of note, visual involvement in GCA includes anterior ischemic optic neuropathy (AION), posterior ischemic optic neuropathy (PION), arterial occlusion, “cotton wool spots” (microinfarcts of the retinal nerve fiber layer), or ocular ischemic syndrome (hypotension, iritis)
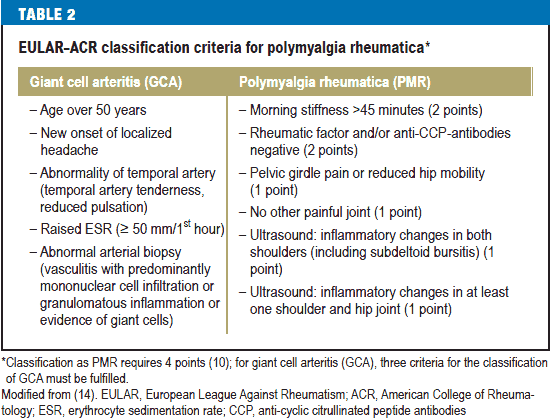
Although classic findings of GCA can be found in a temporal artery biopsy, it is important to remember that GCA is a clinical diagnosis that must be emergently noticed as it can lead to permanent vision loss if not recognized and treated early. EULAR-ACR criteria for diagnosis of GCA are included below for reference:
Since 1949, treatment of GCA mostly consisted of corticosteroids, which may be required for 1-5 years and often results in substantial toxicity – essentially, all patients develop Cushing’s syndrome. In addition, 20-50% of individuals develop other steroid-related toxicity, including fractures, cataracts, peripheral edema, myopathy, infections, and diabetes. Following initial improvement and steroid dose reduction, 1 or more relapses of GCA occur in 27-62% of patients.
We now understand that while steroids and baby aspirin are imperative to initiate immediately upon recognition of GCA, that just as importantly, a steroid-sparing agent should be initiated as well. As Dr. John Stone, Director of Clinical Rheumatology at Massachusetts General Hospital, has been noted to say, “Steroids are the elephant in the room.” But, which steroid-sparing agent should we use? We will review the current literature in reverse chronological order to help answer this question:
2020
In April 2020, Matza et al published in Arthritis Care Res (Hoboken), a prospective, open-label trial of 13 patients treated with subcutaneous ustekinumab (UST)(IL1-12/23i) every 8 weeks + 24 week prednisone taper in patients with active new-onset or relapsing GCA. The trial was stopped prematurely after 7 of the initial 10 patients relapsed.
In 2018, Conway et al published an open-label, prospective study in Seminars Arthritis Rheumatism examining UST for refractory GCA (failed to taper GC despite a median of 1 other immunosuppressive agent) of 25 patients. The study revealed that by week 52, there were significant reductions in GC doses (24% had stopped GC completely), no relapses, decreased CRP levels, and improvement in CTA findings of large vessel vasculitis with use of UST.
2017
The landmark GiACTA trial published in NEJM in 2017 by Stone et al compared weekly tociluzumab (TCZ) + 26 week GC taper vs bi-weekly TCZ + 26 week GC taper vs monotherapy with GC (rapid taper arm of 26 weeks vs long taper arm of 52 weeks). The study revealed that sustained remission at week 52 occurred in 56% of patients on weekly TCZ and that the cumulative median steroid dose was significantly lower in TCZ groups (1.8 g vs 3.8 g). This study included 216 patients from 14 countries with new or relapsing GCA (mean age 69, ~75% female, ~97% Caucasian, ~half with relapsing disease). Also, notably, acute phase reactant levels were not reliable indicators of flares, arguing for reassessment on current clinical practice of laboratory monitoring parameters.
A randomized, double-blind, multicenter trial of Abatacept (CTLA-4Ig) for the treatment of GCA published in 2017 in Arthritis & Rheumatology by Langford et al compared the efficacy of abatacept to placebo in patients with newly diagnosed or relapsing GA who had active disease within the prior 2 months. Eligible patients with active GCA received prednisone (40-60 mg/day) with a standardized taper + abatacept 10 mg/kg IV on D1, 15, 29, and week 8. If the patient was in remission at week 12, then he/she was randomized with double blinded 1:1 treatment assignment to continue abatacept IV every 28 days + GC taper starting at prednisone 20 mg daily or to receive placebo by vein every 28 days + GC taper starting at prednisone 20 mg daily with discontinuation of prednisone at week 28 in both arms and continuation of treatment otherwise in both arms until 12 months after enrollment of the last patient. All such randomized patients (41) were included in the intent to treat analysis. The need to increase prednisone dose or restart prednisone after cessation was considered a relapse criterion. The relapse-free survival at 12 months was 48% for those receiving abatacept and 31% for those receiving placebo and a longer median duration of remission was seen in those receiving abatacept compared to placebo. Although the difference in relapse-free survival rates between treatment arms was statistically and clinically significant despite the small sample size, the small sample size could impact the role of confounding variables within the study.
2002-2013
Prior studies of the TNF-inhibitors infliximab + GC vs placebo + GC (Hoffman et al in the Annals of Internal Medicine in 2007) and adalimumab (Seror et al in the Annals of Rheumatic Disease in 2013) did not show any improvement in relapses or steroid-sparing effect. However, the trial of infliximab for maintenance of GC-induced remission of GCA was too small (44 patients: 28 in study arm, 16 in control arm ) to draw definitive conclusion and only included patients with newly diagnosed GCA. A randomized, double-blind, placebo-controlled trial by Martinez-Taboasa et al in Annals of Rheumatic Disease in 2008 compared etanercept + GC (n = 8, higher ESR rate) with placebo + GC (n = 9) in patients with biopsy-proven GCA and side effects secondary to GC. After 12 months, 50% in the etanercept group and 22% in the placebo group were able to stop GC therapy, but the study did not reach statistical significance. Thus, while it is unclear whether etanercept may have a steroid-sparing effect, this study suggests it may have one.
A multicenter, randomized, double-bind study by Hoffman et al published in Arthritis & Rheumatism in 2002 evaluated treatment with methotrexate (MTX) (median dosage of 15 mg/week) and prednisone (1 mg/kg) in patients with newly diagnosed GCA compared to prednisone alone. The trial showed conflicting results over steroid-sparing effect (steroid doses used in the study were low: 7.5 – 15mg/week) but did show a possible reduction in risk of relapses.
In summary, TCZ has the strongest data behind it for initiation along commencement of GC as a steroid-sparing agent with sustained remission at week 52 in the weekly TCZ arm (56%) and bi-weekly TCZ (53%) compared to rapid GC taper (14%) and prolonged taper (17%).
Future Directions
Fast forward to today where exciting developments are underway.
Specifically, there are 5 trials currently underway evaluating new possibilities for treatment of GCA:
- ABAGART (Abatecept)
- METOGIA (Tociluzumab vs MTX)
- SELECT (Upadacitinib)
- MAVRILIMUMAB (GMCSFi)
- TiTIAN (Seckukinumab)
A great abstract to check out at this year’s meeting is: Abstract Number 1926:






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.