
Search for Terms or Answers
Laure Gossec, 1 Dafna D. Gladman,2 M. Elaine Husni,3 Tadashi Okano,4 Ana-Maria Orbai,5 Fabian Proft,6 Alistair Reid,7 Maarten de Wit,8 Jérémy Lambert,9 Patrick Healy,10 Philip J. Mease11
1 Sorbonne Universite and Pitie-Salpetriere Hospital, Paris, France; 2 University of Toronto, Schroeder Arthritis Institute, Krembil Research Institute, Toronto Western Hospital, Division of Rheumatology, Toronto, Canada; 3 Cleveland Clinic, Department of Rheumatic and Immunologic Diseases, Cleveland, Ohio, USA; 4Osaka Metropolitan University Graduate School of Medicine, Center for Senile Degenerative Disorders (CSDD), Osaka, Japan; 5 Johns Hopkins University School of Medicine, Division of Rheumatology, Baltimore, Maryland, USA; 6Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Department of Gastroenterology, Infectiology and Rheumatology (including Nutrition Medicine), Berlin, Germany; 7 Wollongong Private Hospital (Part of Ramsay Health Care), University of Wollongong, Rheumatology, Wollongong, Australia; 8Stichting Tools, Patient Research Partner, Amsterdam, The Netherlands; 9UCB, Courbevoie, France; 10UCB, Morrisville, USA; 11Providence-Swedish Medical Center and University of Washington, Department of Rheumatology, Seattle, USA.
Abstract or description:Objective
To assess whether achieving stringent treatment responses at Week 16 in bimekizumab (BKZ)-treated patients with active psoriatic arthritis (PsA) was associated with clinically meaningful improvements in patient-reported outcomes (PROs) over 3 years
Background
• PsA is a chronic inflammatory disease in which pain, fatigue and impaired functional capacity are among the most burdensome patient-reported symptoms, each contributing significantly to reduced health-related quality of life.1–3
• Achieving an early and rapid response to treatment is an important goal to reduce symptoms and minimise disease impact.4,5
• BKZ is a monoclonal IgG1 antibody that selectively inhibits interleukin (IL)-17F in addition to IL-17A.
Methods
• BE OPTIMAL (NCT03895203) and BE COMPLETE (NCT03896581) were phase 3 trials, both placebo-controlled to Week 16, which assessed subcutaneous BKZ 160 mg every 4 weeks (Q4W), in patients with active PsA who were biologic disease-modifying antirheumatic drug (bDMARD)-naïve or had prior intolerance or inadequate response to tumour necrosis factor inhibitors (TNFi-IR), respectively.
• Patients completing Week 52 in BE OPTIMAL or Week 16 in BE COMPLETE could enter BE VITAL (open-label extension; NCT04009499), where all patients received BKZ 160 mg Q4W.
• In this post hoc analysis, BKZ-randomised patients were classified as rapid responders or non-responders based on achievement of resolution of swollen joint count (SJC=0) or ≥50% improvement from baseline in American College of Rheumatology response criteria (ACR50) at Week 16.
• The proportion of BKZ-randomised patients reporting clinically meaningful improvements in the following PROs are presented to 3 years (Week 160/148 in BE OPTIMAL or Week 156 in BE COMPLETE), stratified by Week 16 SJC=0 or ACR50 response: – Pain50, defined as a substantial (≥50%) decrease from baseline in pain, measured by visual analogue scale (VAS; score range: 0 [no pain]–100 [most severe pain])6 – FACIT-Fatigue MCID (Functional Assessment of Chronic Illness Therapy-Fatigue minimal clinically important difference; score range 0–52 [higher scores indicate less fatigue]), defined as ≥4-point increase from baseline in patients with FACIT-Fatigue score ≤48 at baseline – PsAID-12 (12-item Psoriatic Arthritis Impact of Disease; score range: 0–10) no symptom or disease impact, defined as PsAID-12 total score ≤1.157
• Data are reported as observed case (OC) or using modified non-responder imputation (mNRI). – mNRI considered all visits following discontinuation due to adverse events or lack of efficacy as non-response; all other missing data were imputed using multiple imputation and the response was derived from the imputed values.
Results
• 431 bDMARD-naïve and 267 TNFi-IR patients were randomised to BKZ in the BE OPTIMAL and BE COMPLETE studies, respectively.
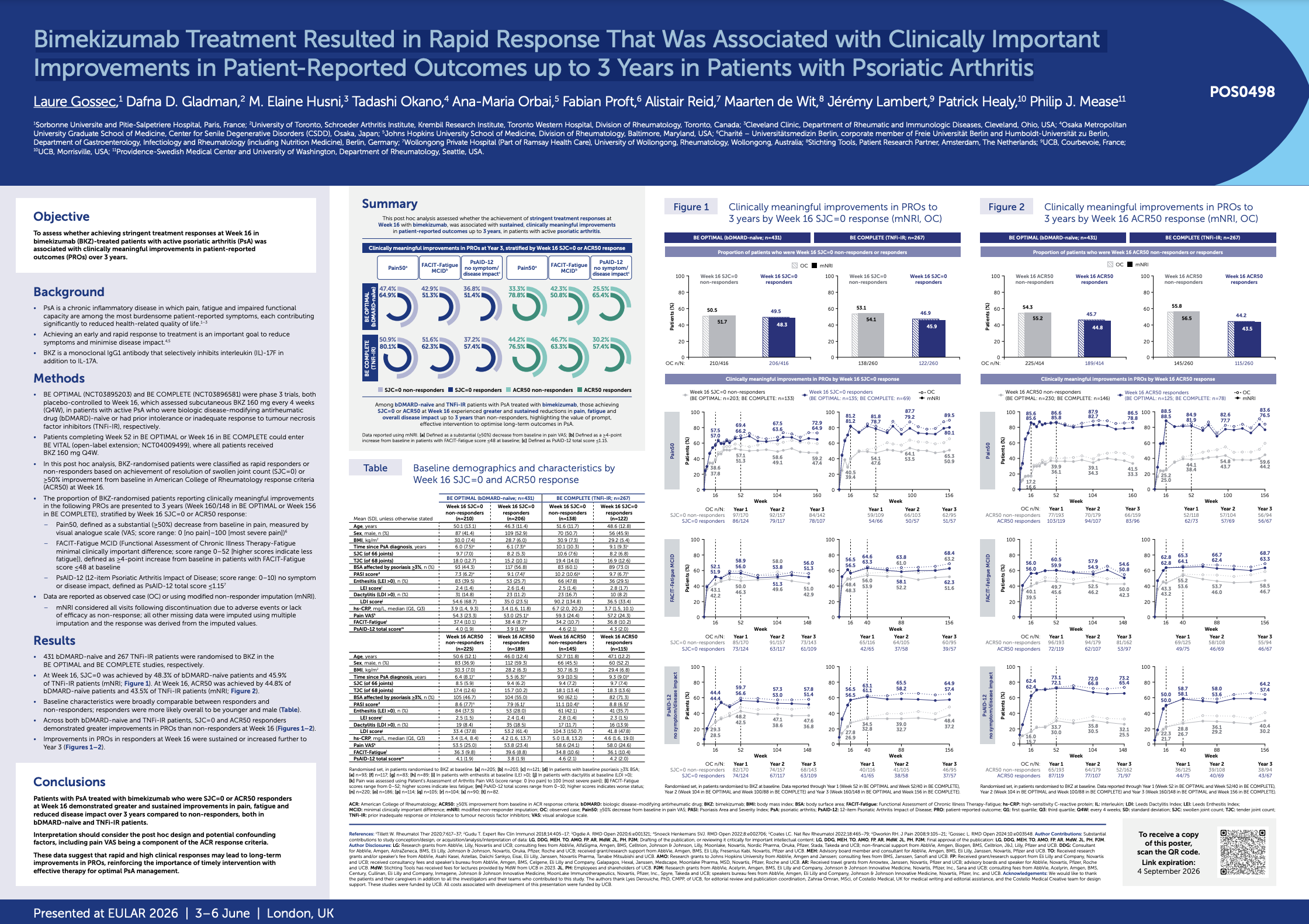
• At Week 16, SJC=0 was achieved by 48.3% of bDMARD-naïve patients and 45.9% of TNFi-IR patients (mNRI; Figure 1). At Week 16, ACR50 was achieved by 44.8% of bDMARD-naïve patients and 43.5% of TNFi-IR patients (mNRI; Figure 2).
• Baseline characteristics were broadly comparable between responders and non-responders; responders were more likely overall to be younger and male (Table).
• Across both bDMARD-naive and TNFi-IR patients, SJC=0 and ACR50 responders demonstrated greater improvements in PROs than non-responders at Week 16 (Figures 1–2).
• Improvements in PROs in responders at Week 16 were sustained or increased further to Year 3 (Figures 1–2).
Conclusions
Patients with PsA treated with bimekizumab who were SJC=0 or ACR50 responders at Week 16 demonstrated greater and sustained improvements in pain, fatigue and reduced disease impact over 3 years compared to non-responders, both in bDMARD-naïve and TNFi-IR patients.
Interpretation should consider the post hoc design and potential confounding factors, including pain VAS being a component of the ACR response criteria.
These data suggest that rapid and high clinical responses may lead to long-term improvements in PROs, reinforcing the importance of timely intervention with effective therapy for optimal PsA managemen
Laure Gossec, 1 Dafna D. Gladman,2 M. Elaine Husni,3 Tadashi Okano,4 Ana-Maria Orbai,5 Fabian Proft,6 Alistair Reid,7 Maarten de Wit,8 Jérémy Lambert,9 Patrick Healy,10 Philip J. Mease11
1 Sorbonne Universite and Pitie-Salpetriere Hospital, Paris, France; 2 University of Toronto, Schroeder Arthritis Institute, Krembil Research Institute, Toronto Western Hospital, Division of Rheumatology, Toronto, Canada; 3 Cleveland Clinic, Department of Rheumatic and Immunologic Diseases, Cleveland, Ohio, USA; 4Osaka Metropolitan University Graduate School of Medicine, Center for Senile Degenerative Disorders (CSDD), Osaka, Japan; 5 Johns Hopkins University School of Medicine, Division of Rheumatology, Baltimore, Maryland, USA; 6Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Department of Gastroenterology, Infectiology and Rheumatology (including Nutrition Medicine), Berlin, Germany; 7 Wollongong Private Hospital (Part of Ramsay Health Care), University of Wollongong, Rheumatology, Wollongong, Australia; 8Stichting Tools, Patient Research Partner, Amsterdam, The Netherlands; 9UCB, Courbevoie, France; 10UCB, Morrisville, USA; 11Providence-Swedish Medical Center and University of Washington, Department of Rheumatology, Seattle, USA.
Abstract or description:Objective
To assess whether achieving stringent treatment responses at Week 16 in bimekizumab (BKZ)-treated patients with active psoriatic arthritis (PsA) was associated with clinically meaningful improvements in patient-reported outcomes (PROs) over 3 years
Background
• PsA is a chronic inflammatory disease in which pain, fatigue and impaired functional capacity are among the most burdensome patient-reported symptoms, each contributing significantly to reduced health-related quality of life.1–3
• Achieving an early and rapid response to treatment is an important goal to reduce symptoms and minimise disease impact.4,5
• BKZ is a monoclonal IgG1 antibody that selectively inhibits interleukin (IL)-17F in addition to IL-17A.
Methods
• BE OPTIMAL (NCT03895203) and BE COMPLETE (NCT03896581) were phase 3 trials, both placebo-controlled to Week 16, which assessed subcutaneous BKZ 160 mg every 4 weeks (Q4W), in patients with active PsA who were biologic disease-modifying antirheumatic drug (bDMARD)-naïve or had prior intolerance or inadequate response to tumour necrosis factor inhibitors (TNFi-IR), respectively.
• Patients completing Week 52 in BE OPTIMAL or Week 16 in BE COMPLETE could enter BE VITAL (open-label extension; NCT04009499), where all patients received BKZ 160 mg Q4W.
• In this post hoc analysis, BKZ-randomised patients were classified as rapid responders or non-responders based on achievement of resolution of swollen joint count (SJC=0) or ≥50% improvement from baseline in American College of Rheumatology response criteria (ACR50) at Week 16.
• The proportion of BKZ-randomised patients reporting clinically meaningful improvements in the following PROs are presented to 3 years (Week 160/148 in BE OPTIMAL or Week 156 in BE COMPLETE), stratified by Week 16 SJC=0 or ACR50 response: – Pain50, defined as a substantial (≥50%) decrease from baseline in pain, measured by visual analogue scale (VAS; score range: 0 [no pain]–100 [most severe pain])6 – FACIT-Fatigue MCID (Functional Assessment of Chronic Illness Therapy-Fatigue minimal clinically important difference; score range 0–52 [higher scores indicate less fatigue]), defined as ≥4-point increase from baseline in patients with FACIT-Fatigue score ≤48 at baseline – PsAID-12 (12-item Psoriatic Arthritis Impact of Disease; score range: 0–10) no symptom or disease impact, defined as PsAID-12 total score ≤1.157
• Data are reported as observed case (OC) or using modified non-responder imputation (mNRI). – mNRI considered all visits following discontinuation due to adverse events or lack of efficacy as non-response; all other missing data were imputed using multiple imputation and the response was derived from the imputed values.
Results
• 431 bDMARD-naïve and 267 TNFi-IR patients were randomised to BKZ in the BE OPTIMAL and BE COMPLETE studies, respectively.
• At Week 16, SJC=0 was achieved by 48.3% of bDMARD-naïve patients and 45.9% of TNFi-IR patients (mNRI; Figure 1). At Week 16, ACR50 was achieved by 44.8% of bDMARD-naïve patients and 43.5% of TNFi-IR patients (mNRI; Figure 2).
• Baseline characteristics were broadly comparable between responders and non-responders; responders were more likely overall to be younger and male (Table).
• Across both bDMARD-naive and TNFi-IR patients, SJC=0 and ACR50 responders demonstrated greater improvements in PROs than non-responders at Week 16 (Figures 1–2).
• Improvements in PROs in responders at Week 16 were sustained or increased further to Year 3 (Figures 1–2).
Conclusions
Patients with PsA treated with bimekizumab who were SJC=0 or ACR50 responders at Week 16 demonstrated greater and sustained improvements in pain, fatigue and reduced disease impact over 3 years compared to non-responders, both in bDMARD-naïve and TNFi-IR patients.
Interpretation should consider the post hoc design and potential confounding factors, including pain VAS being a component of the ACR response criteria.
These data suggest that rapid and high clinical responses may lead to long-term improvements in PROs, reinforcing the importance of timely intervention with effective therapy for optimal PsA managemen
By downloading this material, I acknowledge that it may be used only for personal use and personal education and that I will accredit RheumNow.com as the source and owner of this material. Commercial use or mass reproduction of this material without permission from RheumNow (info@rheumnow.com) is prohibited.