
Search for Terms or Answers
Joseph F. Merola,1 Laure Gossec,2 April W. Armstrong,3 Lourdes Pérez-Chada,4 Jose U. Scher,5 Carle Paul,6 Michael Plewinski,7 Bharat Suryawanshi,7 Charo Scott,7 Stefan Varga,7 Philip J. Mease8
1Department of Dermatology and Department of Medicine, Division of Rheumatology, Peter O'Donnell Jr School of Public Health, The University of Texas Southwestern Medical Center, Dallas, TX, USA; 2Sorbonne Université, Pitié-Salpêtrière Hospital, Paris, France; 3University of California, Los Angeles, Los Angeles, CA, USA; 4Department of Dermatology, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA; 5Department of Medicine, Division of Rheumatology, NYU Grossman School of Medicine, and NYU Psoriatic Arthritis Center, NYU Langone Health, New York, NY, USA; 6Department of Dermatology, INSERM Infinity, Toulouse University, Toulouse, France; 7Bristol Myers Squibb, Princeton, NJ, USA; 8Providence Swedish Medical Center and University of Washington, Seattle, WA, USA
Abstract or description:Background
Deucravacitinib is a selective, oral tyrosine kinase 2 (TYK2) inhibitor with an established clinical profile in moderate to severe plaque psoriasis, supported by over 5 years of follow-up and approval in multiple countries for that indication.1 In 2 randomized, double-blind 52-week phase 3 trials of active psoriatic arthritis (POETYK PsA-1 [NCT04908202] and PsA-2 [NCT04908189]), deucravacitinib demonstrated superior efficacy vs placebo at week 16, with responses maintained through week 52.2,3 This post hoc pooled analysis of POETYK PsA-1 and PsA-2 evaluated efficacy and safety of deucravacitinib at week 52 in relation to concomitant methotrexate use.
Objectives
To evaluate the impact of concomitant methotrexate use on clinical efficacy, patient-reported outcomes, and safety observed at week 52 in patients treated with deucravacitinib using pooled data from the POETYK PsA-1 and PsA-2 trials.
Methods
In POETYK PsA-1 and PsA-2, patients were randomized 1:1 to receive deucravacitinib 6 mg once daily or placebo through week 16. At week 16, patients initially receiving deucravacitinib continued treatment, while those receiving placebo switched to deucravacitinib through week 52. For this post hoc analysis, efficacy data at week 52 were pooled from POETYK PsA-1 and PsA-2 for patients who received continuous deucravacitinib. Binary endpoints were analyzed using Fisher exact test, with nonresponder imputation for missing data. Continuous endpoints were assessed using an independent-sample t test. Safety data, including adverse events (AEs) and serious AEs, were evaluated in all patients who received deucravacitinib through week 52. Incidence rate per 100 person-years of exposure (IR/100 PY) was calculated. The cumulative treatment period included events that occurred after deucravacitinib administration began. All P values were descriptive.
Results
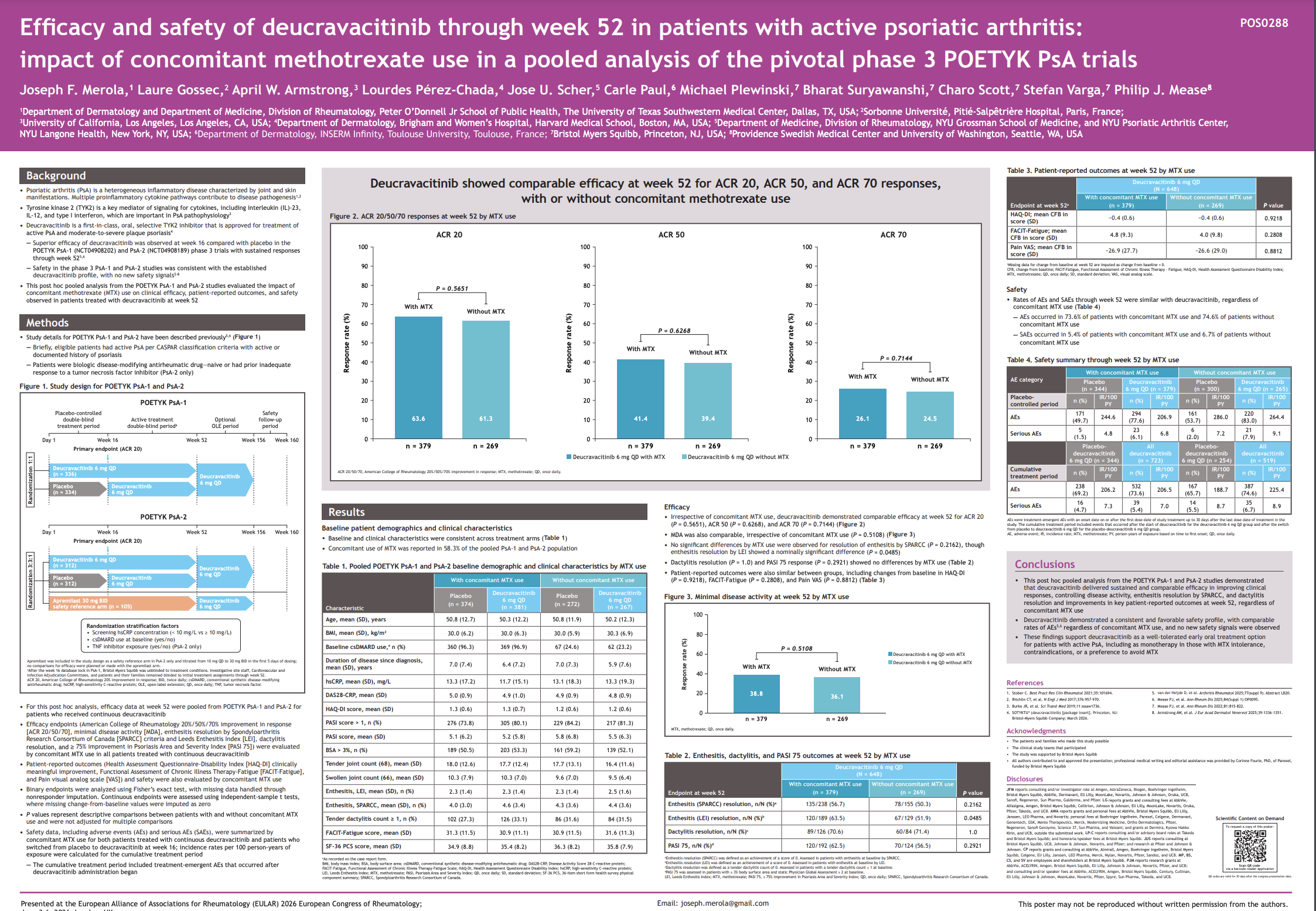
In 648 patients treated with continuous deucravacitinib, the mean (SD) age was 50.2 (12.2), 48.9% were female, and 66.5% used conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) at baseline. In 646 patients treated with placebo through week 16 who switched to deucravacitinib through week 52, the mean (SD) age was 50.8 (12.3), 52.3% were female, and 66.1% used csDMARDs at baseline. At week 52, treatment with continuous deucravacitinib demonstrated comparable efficacy with and without concomitant methotrexate use for American College of Rheumatology 20%/50%/70% improvement in response (ACR 20: with methotrexate, 63.6%; without methotrexate, 61.3%; P = 0.57; ACR 50: with methotrexate, 41.4%; without methotrexate, 39.4%; P = 0.63; ACR 70: with methotrexate, 26.1%; without methotrexate, 24.5%; P = 0.71) and minimal disease activity (MDA: with methotrexate, 38.8%; without methotrexate, 36.1%; P = 0.51). No significant differences by methotrexate use were observed for enthesitis resolution by Spondyloarthritis Research Consortium of Canada (SPARCC) criteria (with methotrexate, 56.7%; without methotrexate, 50.3%; P = 0.22), dactylitis resolution (with methotrexate, 70.6%; without methotrexate, 71.4%; P = 1.00), or ≥ 75% improvement in the Psoriasis Area and Severity Index (PASI 75: with methotrexate, 62.5%; without methotrexate, 56.5%; P = 0.29). Patient-reported outcomes were also similar between groups, including clinically meaningful improvement in Health Assessment Questionnaire Disability Index (HAQ-DI: with methotrexate, 55.8%; without methotrexate, 53.1%; P = 0.55), and change from baseline in Functional Assessment of Chronic Illness Therapy - Fatigue (FACIT-Fatigue: with methotrexate, 5.5; without methotrexate, 4.8; P = 0.43), and visual analog scale of pain (Pain VAS: with methotrexate, −31.1; without methotrexate, −32.4; P = 0.61). Safety did not differ by methotrexate use. During the cumulative treatment period, AEs occurred in 73.6% of patients with concomitant methotrexate use and 74.6% of patients without concomitant methotrexate use; serious AEs occurred in 5.4% and 6.7% of patients, respectively.
Conclusions
Regardless of concomitant methotrexate use, deucravacitinib delivered sustained and comparable efficacy for key clinical endpoints, including ACR responses, optimal control of disease activity (MDA), enthesitis and dactylitis resolution, and improvements in key patient-reported outcomes. Safety was favorable with deucravacitinib and similar with or without methotrexate. No new safety signals were observed, reinforcing the tolerability profile. Results from this post hoc analysis underscore the efficacy and safety of deucravacitinib independent of methotrexate use and may offer an alternative oral treatment option for patients with active PsA with or without intolerance of, or contraindications to, methotrexate.
References
1. Armstrong AW, et al. J of Skin 2025;9:s532.
2. van der Heijde D, et al. Arthritis Rheumatol 2025;77(suppl 9). Abstract LB20.
3. Mease PJ, et al. Ann Rheum Dis 2025;84:84–85. Abstract OP0095.
This Abstract was accepted for publication by the European Alliance of Associations for Rheumatology (EULAR; June 3-6, 2026; London).
Joseph F. Merola,1 Laure Gossec,2 April W. Armstrong,3 Lourdes Pérez-Chada,4 Jose U. Scher,5 Carle Paul,6 Michael Plewinski,7 Bharat Suryawanshi,7 Charo Scott,7 Stefan Varga,7 Philip J. Mease8
1Department of Dermatology and Department of Medicine, Division of Rheumatology, Peter O'Donnell Jr School of Public Health, The University of Texas Southwestern Medical Center, Dallas, TX, USA; 2Sorbonne Université, Pitié-Salpêtrière Hospital, Paris, France; 3University of California, Los Angeles, Los Angeles, CA, USA; 4Department of Dermatology, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA; 5Department of Medicine, Division of Rheumatology, NYU Grossman School of Medicine, and NYU Psoriatic Arthritis Center, NYU Langone Health, New York, NY, USA; 6Department of Dermatology, INSERM Infinity, Toulouse University, Toulouse, France; 7Bristol Myers Squibb, Princeton, NJ, USA; 8Providence Swedish Medical Center and University of Washington, Seattle, WA, USA
Abstract or description:Background
Deucravacitinib is a selective, oral tyrosine kinase 2 (TYK2) inhibitor with an established clinical profile in moderate to severe plaque psoriasis, supported by over 5 years of follow-up and approval in multiple countries for that indication.1 In 2 randomized, double-blind 52-week phase 3 trials of active psoriatic arthritis (POETYK PsA-1 [NCT04908202] and PsA-2 [NCT04908189]), deucravacitinib demonstrated superior efficacy vs placebo at week 16, with responses maintained through week 52.2,3 This post hoc pooled analysis of POETYK PsA-1 and PsA-2 evaluated efficacy and safety of deucravacitinib at week 52 in relation to concomitant methotrexate use.
Objectives
To evaluate the impact of concomitant methotrexate use on clinical efficacy, patient-reported outcomes, and safety observed at week 52 in patients treated with deucravacitinib using pooled data from the POETYK PsA-1 and PsA-2 trials.
Methods
In POETYK PsA-1 and PsA-2, patients were randomized 1:1 to receive deucravacitinib 6 mg once daily or placebo through week 16. At week 16, patients initially receiving deucravacitinib continued treatment, while those receiving placebo switched to deucravacitinib through week 52. For this post hoc analysis, efficacy data at week 52 were pooled from POETYK PsA-1 and PsA-2 for patients who received continuous deucravacitinib. Binary endpoints were analyzed using Fisher exact test, with nonresponder imputation for missing data. Continuous endpoints were assessed using an independent-sample t test. Safety data, including adverse events (AEs) and serious AEs, were evaluated in all patients who received deucravacitinib through week 52. Incidence rate per 100 person-years of exposure (IR/100 PY) was calculated. The cumulative treatment period included events that occurred after deucravacitinib administration began. All P values were descriptive.
Results
In 648 patients treated with continuous deucravacitinib, the mean (SD) age was 50.2 (12.2), 48.9% were female, and 66.5% used conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) at baseline. In 646 patients treated with placebo through week 16 who switched to deucravacitinib through week 52, the mean (SD) age was 50.8 (12.3), 52.3% were female, and 66.1% used csDMARDs at baseline. At week 52, treatment with continuous deucravacitinib demonstrated comparable efficacy with and without concomitant methotrexate use for American College of Rheumatology 20%/50%/70% improvement in response (ACR 20: with methotrexate, 63.6%; without methotrexate, 61.3%; P = 0.57; ACR 50: with methotrexate, 41.4%; without methotrexate, 39.4%; P = 0.63; ACR 70: with methotrexate, 26.1%; without methotrexate, 24.5%; P = 0.71) and minimal disease activity (MDA: with methotrexate, 38.8%; without methotrexate, 36.1%; P = 0.51). No significant differences by methotrexate use were observed for enthesitis resolution by Spondyloarthritis Research Consortium of Canada (SPARCC) criteria (with methotrexate, 56.7%; without methotrexate, 50.3%; P = 0.22), dactylitis resolution (with methotrexate, 70.6%; without methotrexate, 71.4%; P = 1.00), or ≥ 75% improvement in the Psoriasis Area and Severity Index (PASI 75: with methotrexate, 62.5%; without methotrexate, 56.5%; P = 0.29). Patient-reported outcomes were also similar between groups, including clinically meaningful improvement in Health Assessment Questionnaire Disability Index (HAQ-DI: with methotrexate, 55.8%; without methotrexate, 53.1%; P = 0.55), and change from baseline in Functional Assessment of Chronic Illness Therapy - Fatigue (FACIT-Fatigue: with methotrexate, 5.5; without methotrexate, 4.8; P = 0.43), and visual analog scale of pain (Pain VAS: with methotrexate, −31.1; without methotrexate, −32.4; P = 0.61). Safety did not differ by methotrexate use. During the cumulative treatment period, AEs occurred in 73.6% of patients with concomitant methotrexate use and 74.6% of patients without concomitant methotrexate use; serious AEs occurred in 5.4% and 6.7% of patients, respectively.
Conclusions
Regardless of concomitant methotrexate use, deucravacitinib delivered sustained and comparable efficacy for key clinical endpoints, including ACR responses, optimal control of disease activity (MDA), enthesitis and dactylitis resolution, and improvements in key patient-reported outcomes. Safety was favorable with deucravacitinib and similar with or without methotrexate. No new safety signals were observed, reinforcing the tolerability profile. Results from this post hoc analysis underscore the efficacy and safety of deucravacitinib independent of methotrexate use and may offer an alternative oral treatment option for patients with active PsA with or without intolerance of, or contraindications to, methotrexate.
References
1. Armstrong AW, et al. J of Skin 2025;9:s532.
2. van der Heijde D, et al. Arthritis Rheumatol 2025;77(suppl 9). Abstract LB20.
3. Mease PJ, et al. Ann Rheum Dis 2025;84:84–85. Abstract OP0095.
This Abstract was accepted for publication by the European Alliance of Associations for Rheumatology (EULAR; June 3-6, 2026; London).
By downloading this material, I acknowledge that it may be used only for personal use and personal education and that I will accredit RheumNow.com as the source and owner of this material. Commercial use or mass reproduction of this material without permission from RheumNow (info@rheumnow.com) is prohibited.