All News

RA Patients on Biologics and tsDMARDs are still High Risk
A new Swedish ARTIS registry study of key safety outcomes in rheumatoid arthritis (RA) patients receiving either targeted synthetic or biological disease-modifying antirheumatic drugs (b/ts DMARDs, including Janus Kinase inhibitors (JAKi)), has been updated and affirms previously held risks.
Read Article
EMA Final Update on JAK Inhibitors and MACE, Malignancy & VTE Risks
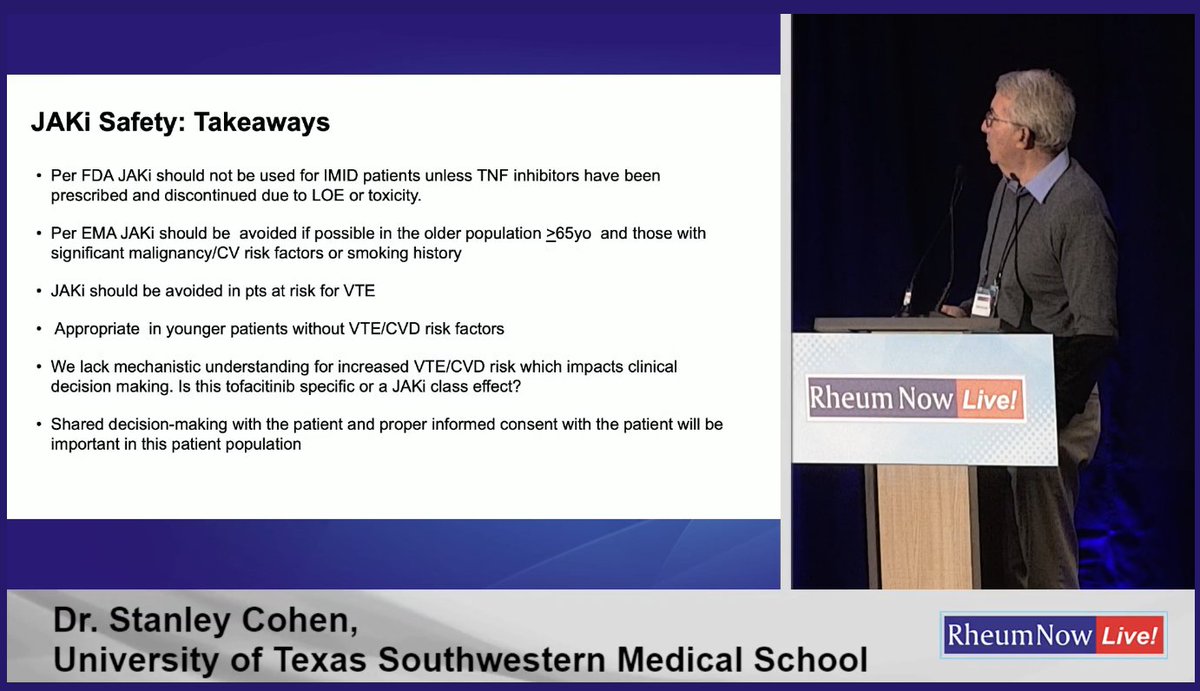
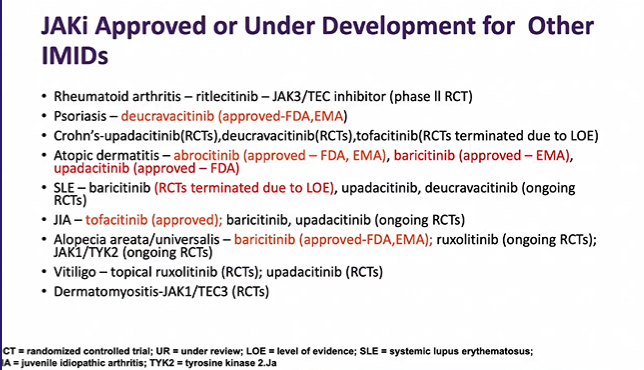
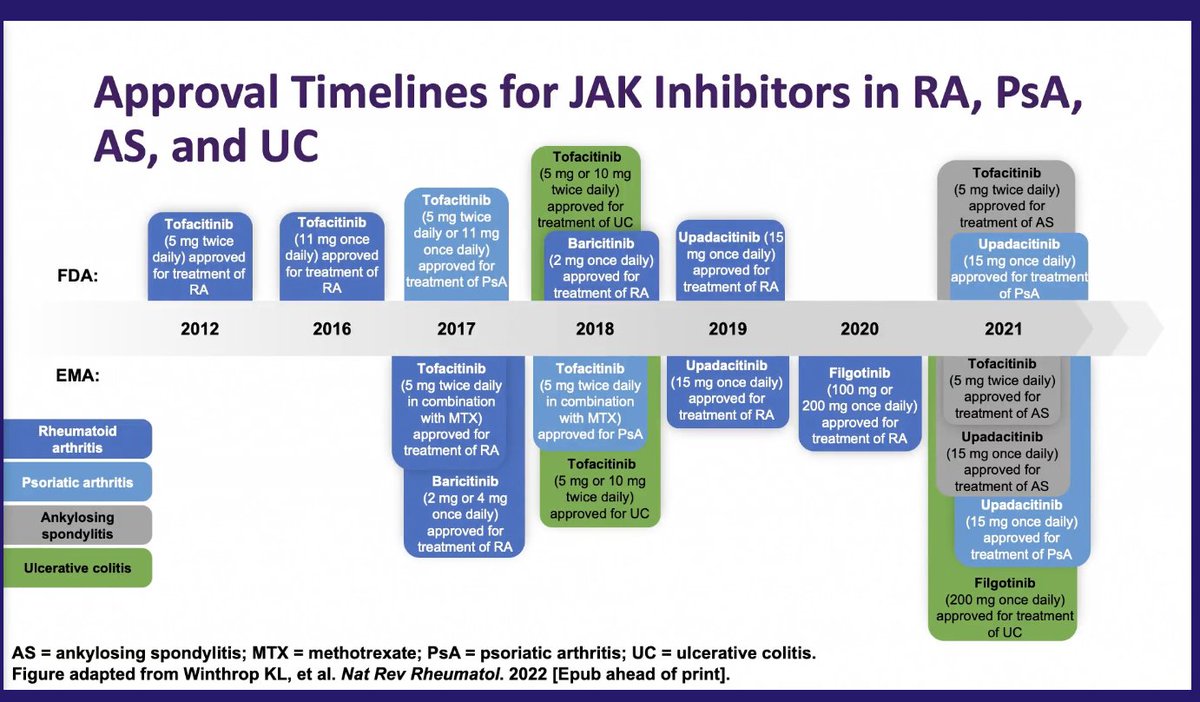
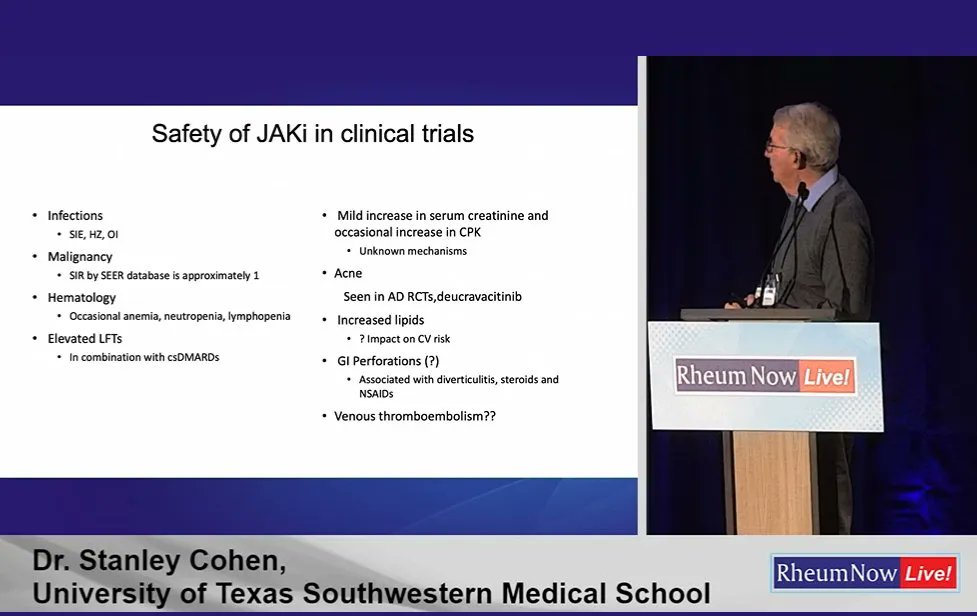
The EMA has updated recommendations regarding the use of JAK inhibitors by issuing a direct healthcare professional communication summarizing the data and warnings regarding an increased risk of malignancy, major adverse cardiovascular events (MACE), serious infections, VTE, and mortality in some patients receiving JAKi for the treatment of chronic inflammatory disorders.
Read Article
Night Splinting for Carpal Tunnel (3.24.2023)
Dr. Jack Cush reviews the news and journal articles from the past 2 weeks on RheumNow.com. This week reviews clinical associations with SS-A, a new biomarker for SSc-ILD and cancer screening for myositis patients.
Read Article
Links:

Links:

Links:

Links:

Links:
Links:
Links: