All News
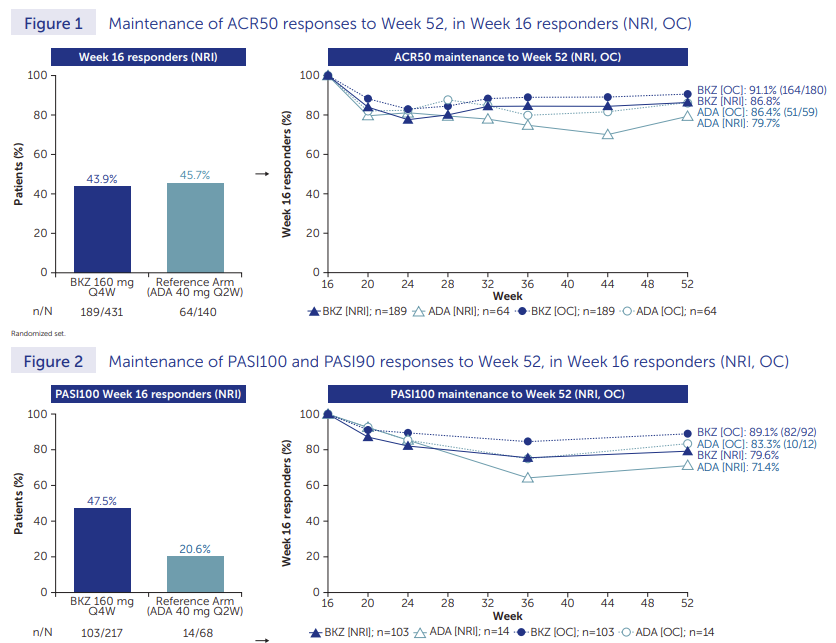
Rather unsurprising finding at this point, but valuable nonetheless
Per usual, joint efficacy for bimekizumab (IL17i) ~similar to TNF
New twist; similar loss in efficacy over time. Nice to have another IL17i; not sure this is a "blockbuster"
@RheumNow #ACR23 Abstr1437 https://t.co/4sVfSz7ZnK
Mike Putman EBRheum ( View Tweet)
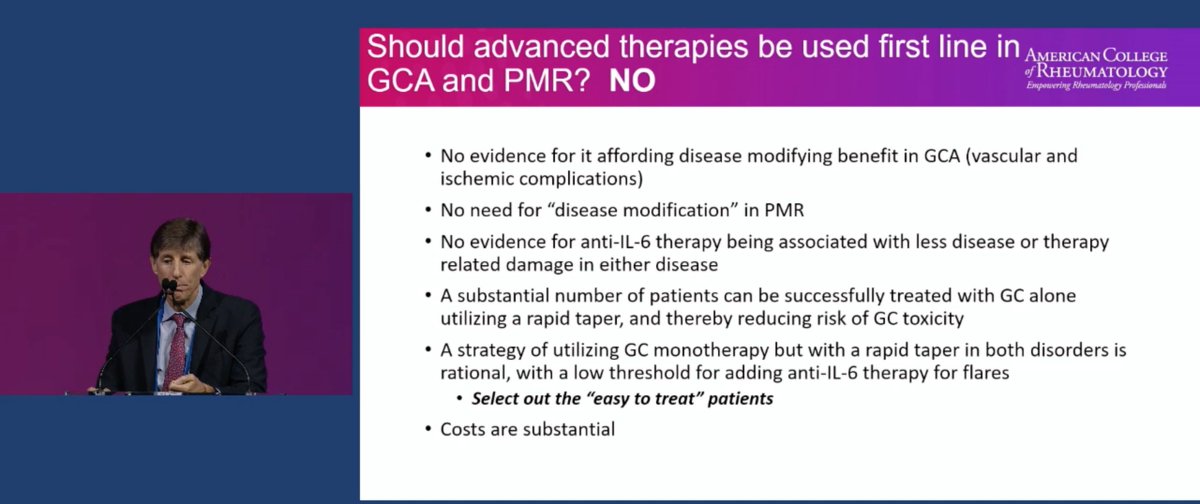
Great Debate on the use of biologics in treatment of Giant Cell Arteritis and Polymyalgia Rheumatica!
Let's begin with Dr. Robert Spiera on why we should NOT use IL-6i
No evidence of disease modifying
Lose biomarker activity
Cost
@RheumNow #ACR23 #ACRbest https://t.co/XCT02wYb2s
Robert B Chao, MD ( View Tweet)
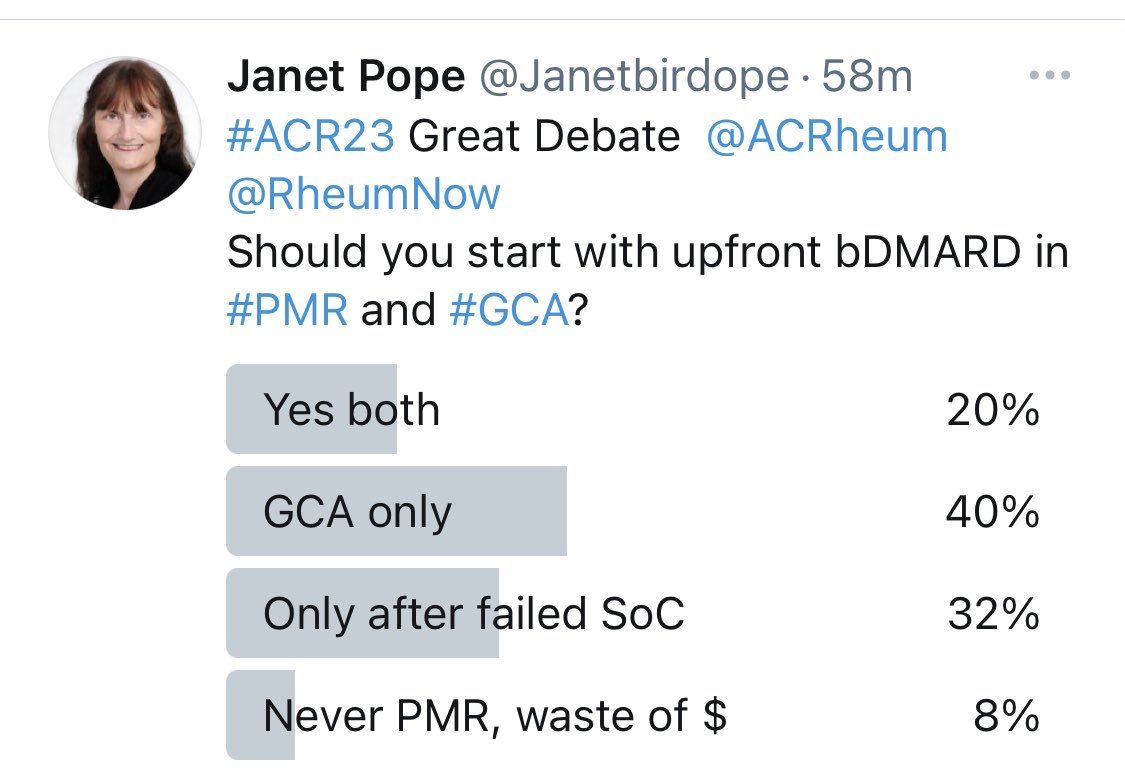
Here is the popular answer@to the #ACR23 debate of up front bDMARD in GCA and PMR Yes vs No. the audience has no consensus. Access is Impt, experience and criteria of who to use it in. @ACRheum @RheumNow https://t.co/7pxF4w926m
Janet Pope ( View Tweet)

Debaters and moderators acknowledge IL6i may not be the only steroid sparing agents that would work for #GCA. Abatacept, secukinumab, JAKi are being evaluated #greatdebate @rheumnow #ACR23
TheDaoIndex KDAO2011 ( View Tweet)

The order of use will affect the safety and effectiveness of drug Rx in #Rheumatoid #arthritis So if #Rituximab is used in later line #Rx - is looks worse@than ex #TNFi used early. Never forget prescribing bias / confounding the results. @RheumNow @ACRheum #ACR23 https://t.co/JJ8BY7n9VM
Janet Pope ( View Tweet)

More nuanced poll for #GreatDebate #ACR23
@RheumNow
How should we use biologics for PMR/GCA?
Eric Dein ( View Tweet)
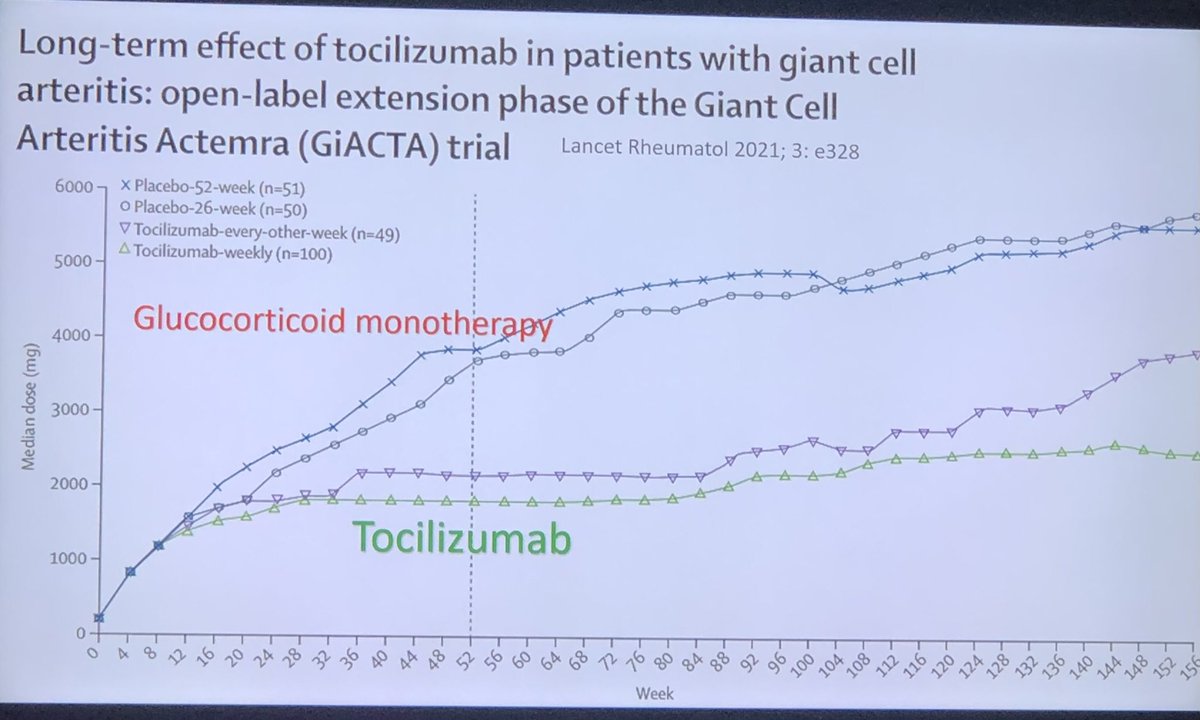
#GCA Rx #bDMARD is established to #steroid spare and reduce relapses. #Tocilizumab #GiACTA Dr Seo said ‘biologics work and steroids are bad!’ @ACRheum @RheumNow #ACR23 #ACRbest https://t.co/JmSE1KKlf5
Janet Pope ( View Tweet)
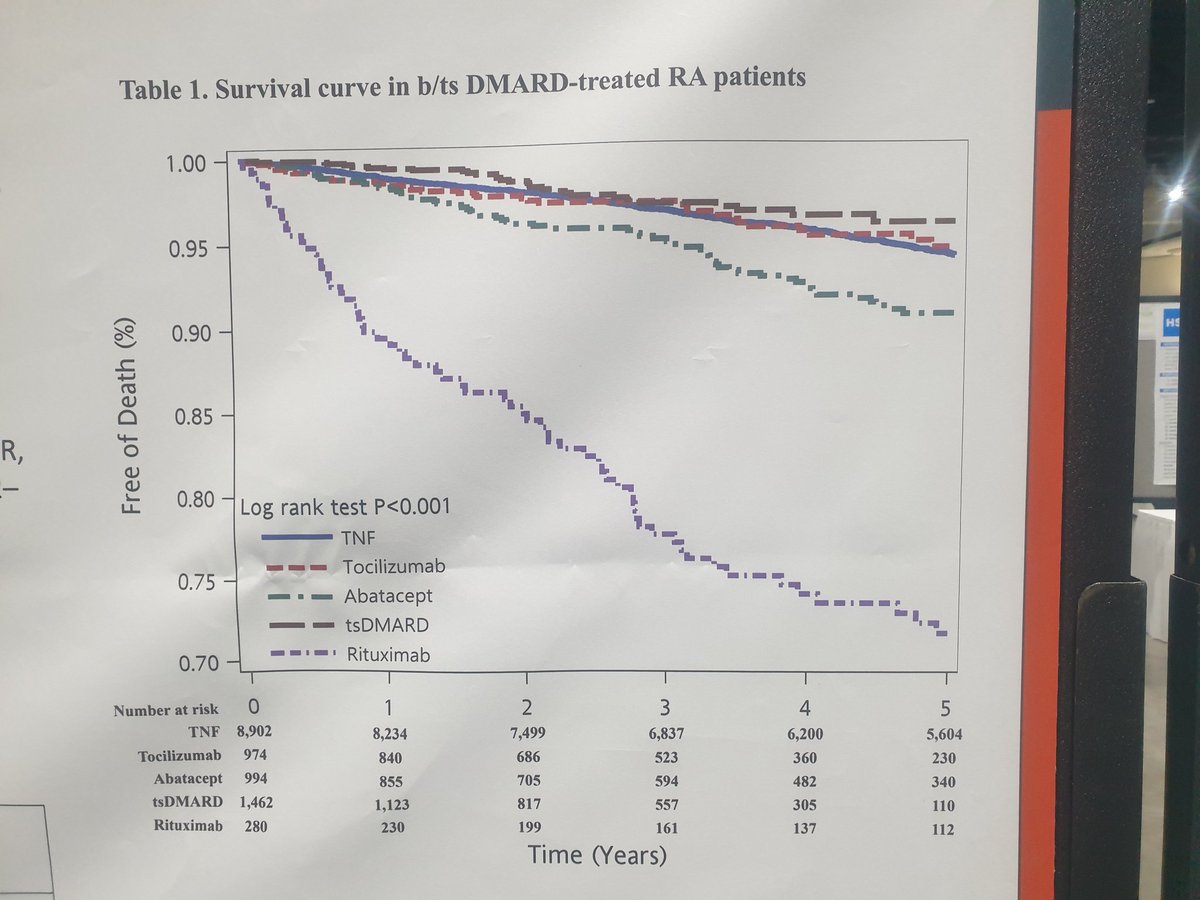
Taiwanaise study of factors associated with 5 year mortality in patients after their first biological b,ts DMARDS
A highter risque mortality in RTX and lower in tsDMARD vs TNFi @RheumNow @Janetbirdope @Yuz6Yusof https://t.co/rjpo08Tg46
Dellal ( View Tweet)
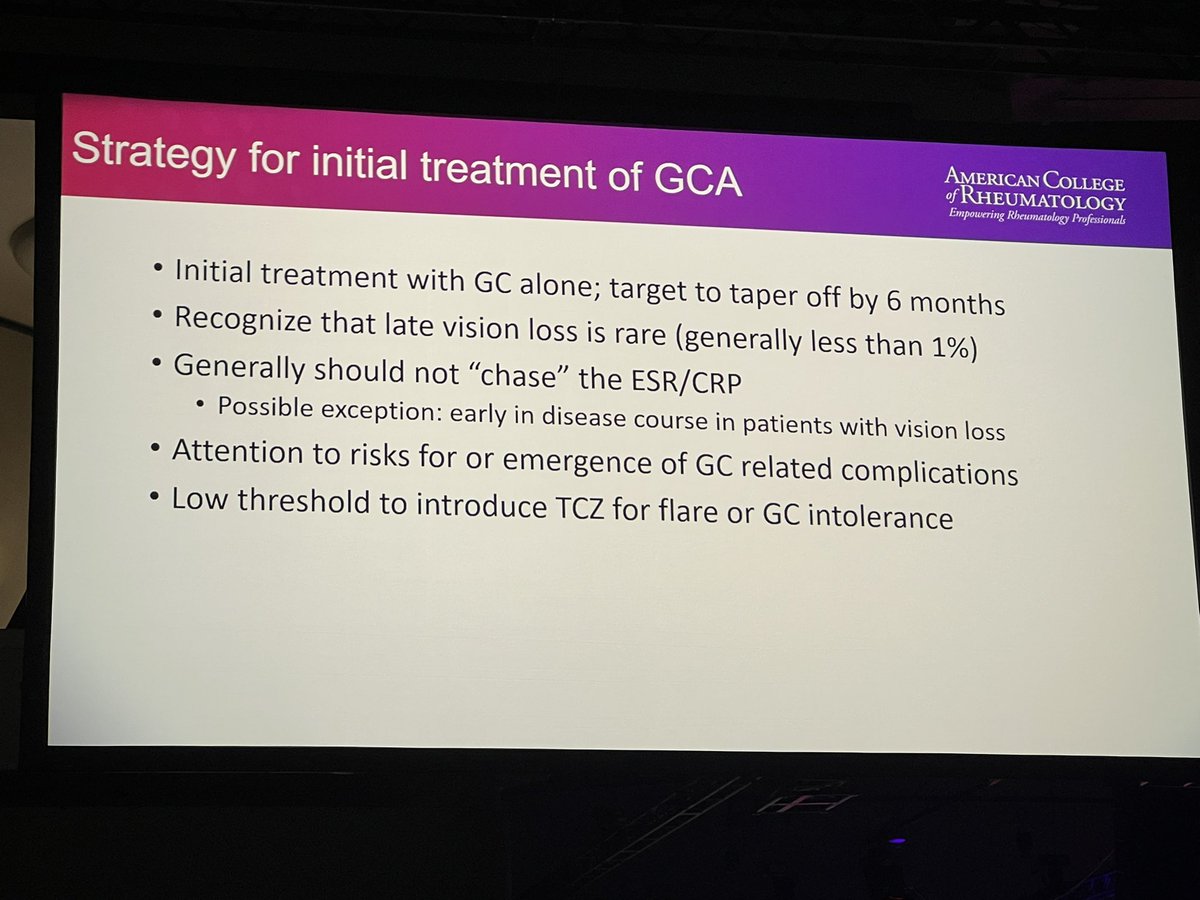
#ACR23 Great debate: should we use biologics at PMR/GCA onset?
Dr Spiera (Cons)
-Need to agree on clin important diff & flares
-No evidence as disease modifying in GCA
- No need for disease modifying in PMR
-Most pts can be treated with steroid & rapid taper
-Cost @RheumNow https://t.co/ptM8E7EQzF
Md Yuzaiful Md Yusof ( View Tweet)
#ACR23 Great Debate @ACRheum @RheumNow
Should you start with upfront bDMARD in #PMR and #GCA?
Janet Pope ( View Tweet)
Real World SLE Rx patterns from the SPOCS cohort. 70+% IFN high, 81% on antimalarials, 21% biologics, and 55% IS, 65% GCs. High IFN pts had more IS and steroid use. 45+% still on GCs at 12 months despite avail of new therapeutics @RheumNow #ACR23 abst#0592
TheDaoIndex KDAO2011 ( View Tweet)
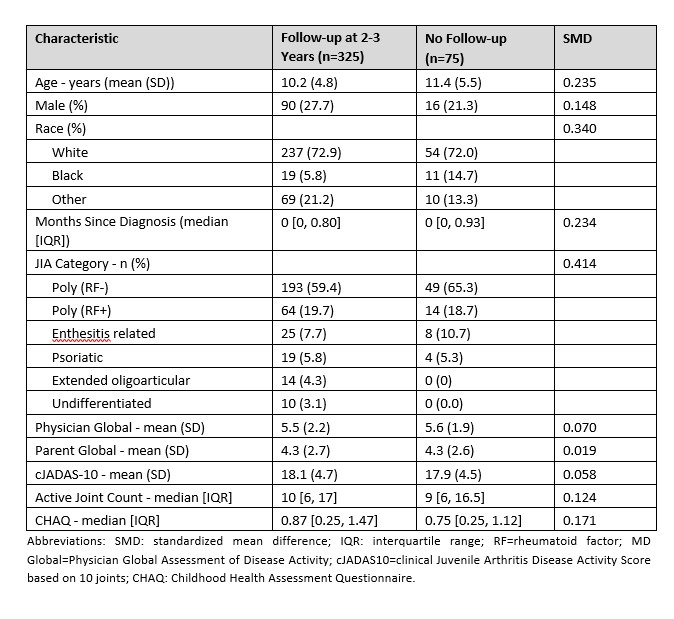
STOP-JIA study data from Abs #0831 suggest improved effectiveness with early combination tx vs step up and biologic first tx at the 2-3 yr timeframe for pJIA pts. More data needed to optimize outcomes/tx for these children. https://t.co/vWL5J4FPbo #ACR23 @rheumnow https://t.co/5iJpwglhPu
Dr. Rachel Tate ( View Tweet)
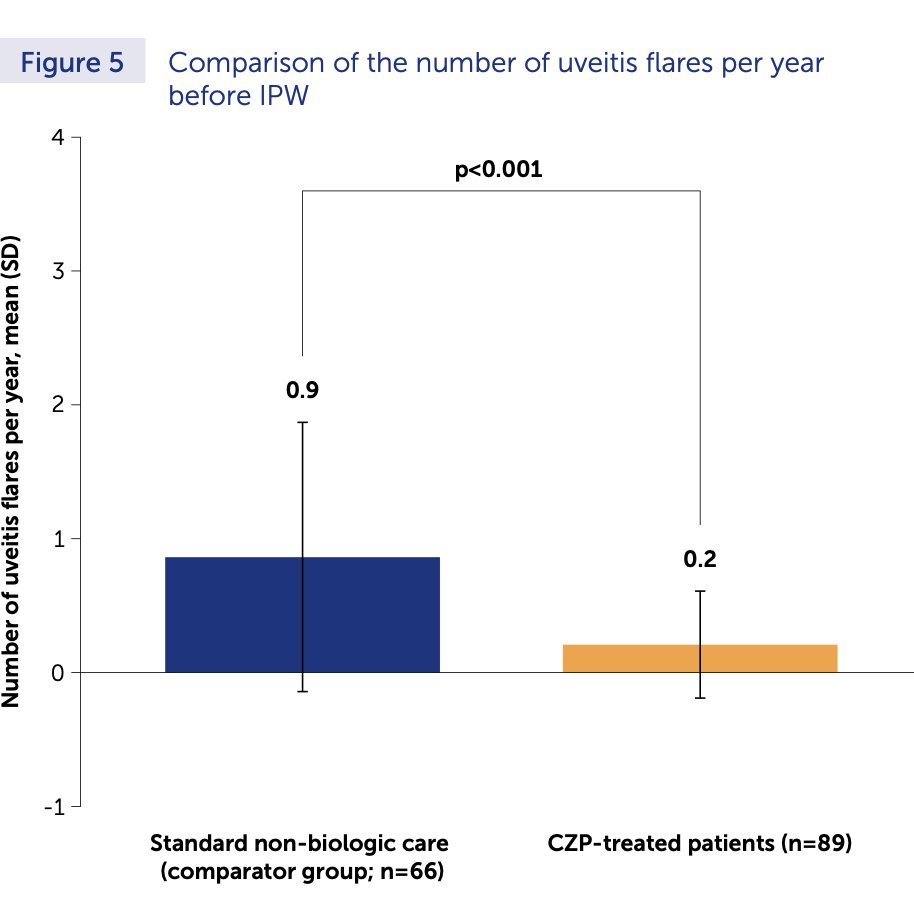
ABS0524:
⭐️Benefit of Certolizumab (CZP) over standard non-biologic tx in reducing acute anterior uveitis (AAU) flares among high risk pts w/ axSpA
➡️active dz, HLAB27+, 2 or more AAU flares
⭐️CZP reduced AAU flare rate by 87%
#ACR23 @RheumNow
#ACRBest https://t.co/rW0N18agMO
Meral K. El Ramahi, MD MeralElRamahiMD ( View Tweet)
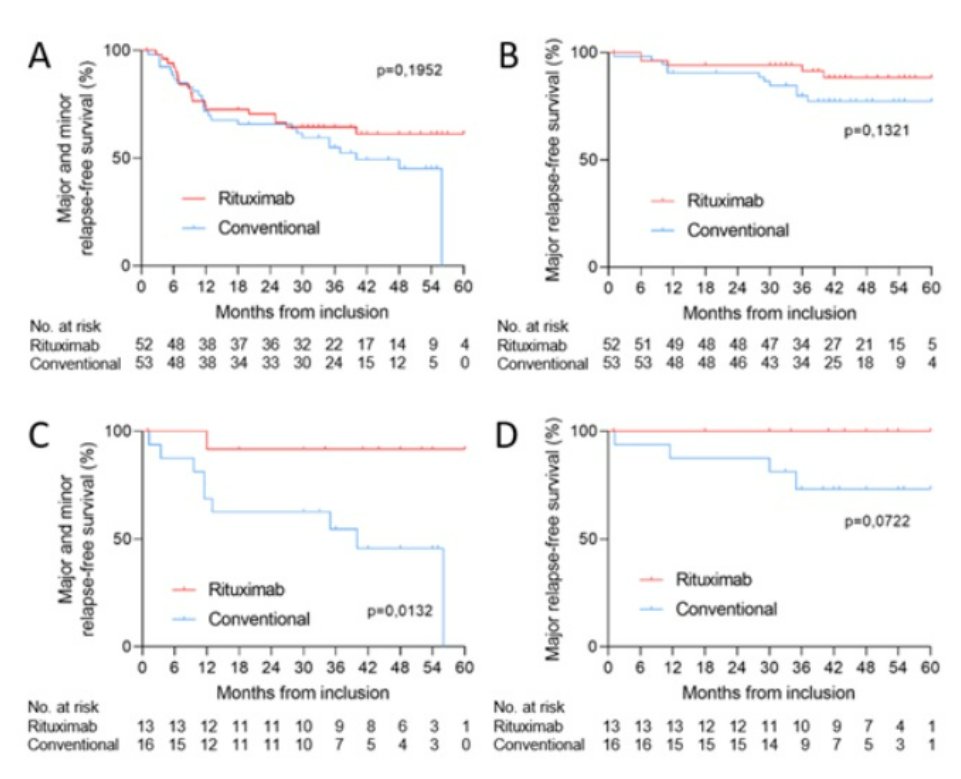
LTE of REOVAS of RTX in EGPA. Relapse free survival 64% vs 51%, major relapse free 90% vs 79%. If MPO+ relapse free survival 92% vs 50%. Abstr#0854 #ACR23 @RheumNow https://t.co/76hlYRxWhY https://t.co/RSsgxxQKVC
Richard Conway ( View Tweet)
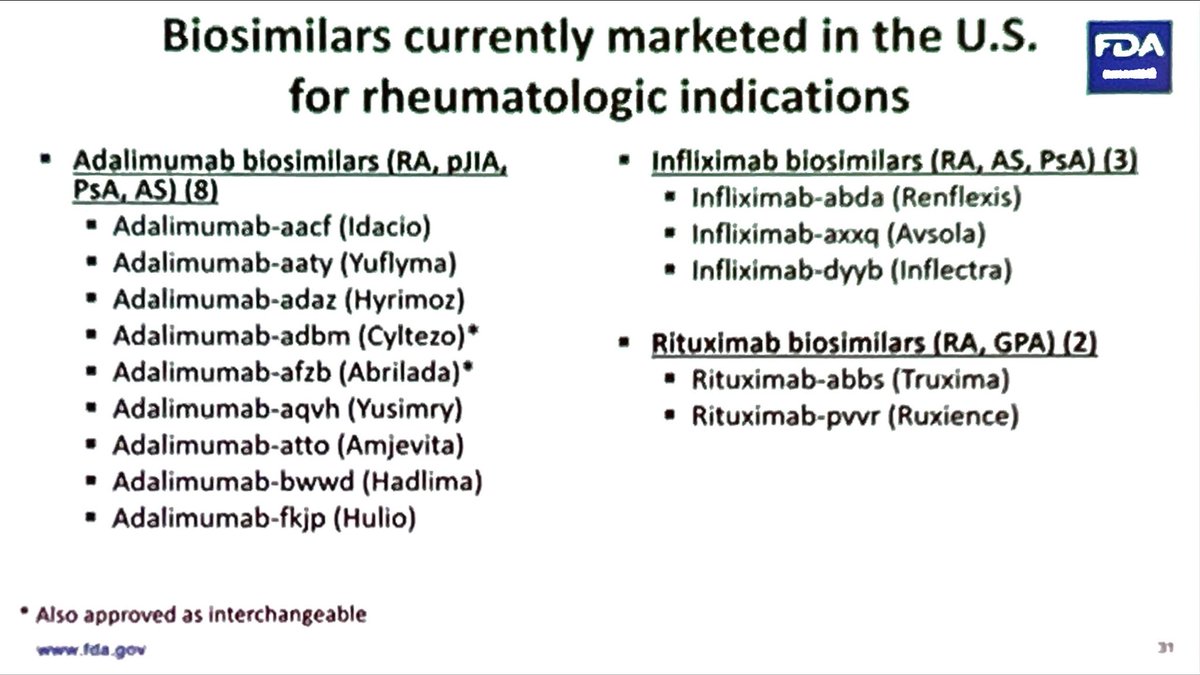
The critical mass of biosimilars in the US is surely getting there.
My opinion: now it’s time for price competition. Otherwise you have to ask, what was the point of it all?
Maybe I’m just a naive foreigner. But US patients deserve better.
#ACR23 @US_FDA session @RheumNow https://t.co/enHY6xffMa
David Liew drdavidliew ( View Tweet)
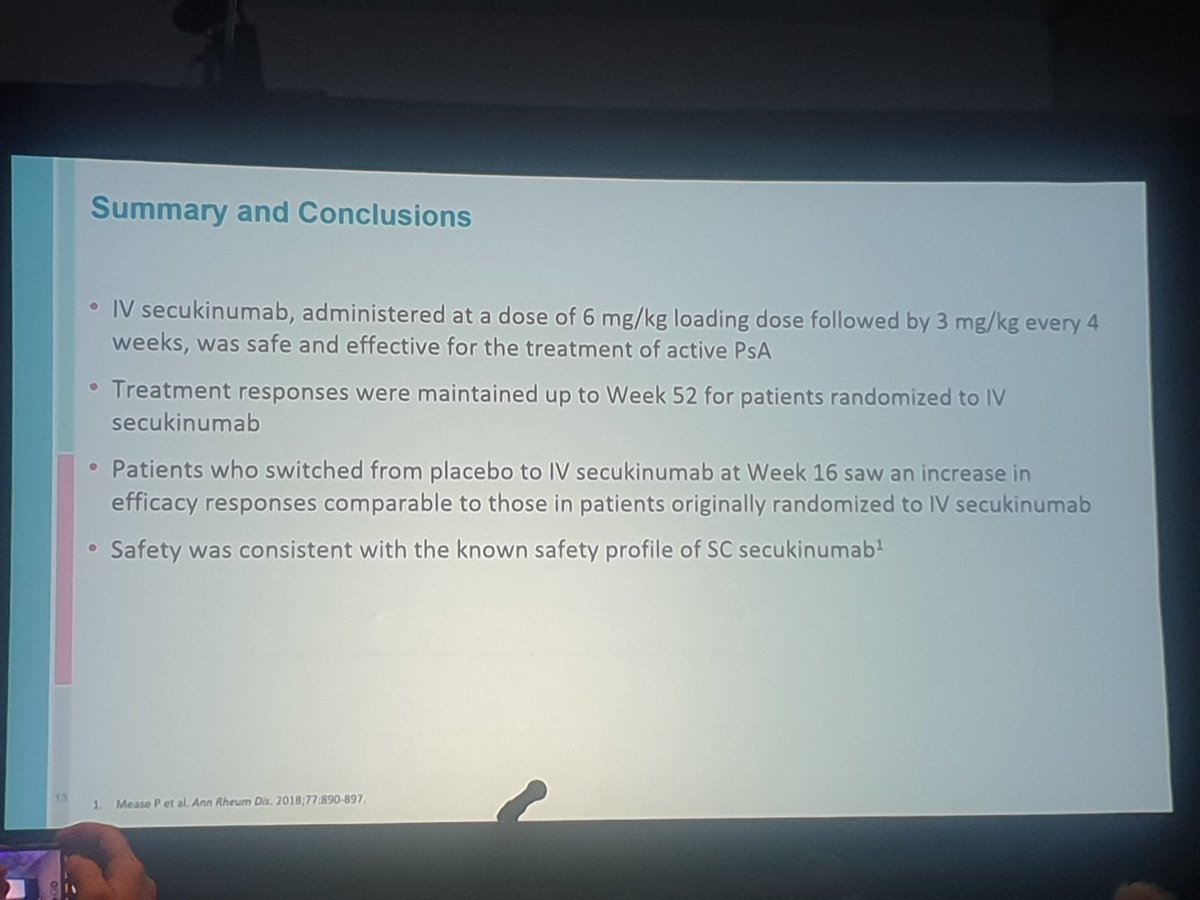
#ACR23
IV secukinumab vs placebo at 52 Weeks
@RheumNow https://t.co/4zQa37tN4l
Dellal ( View Tweet)
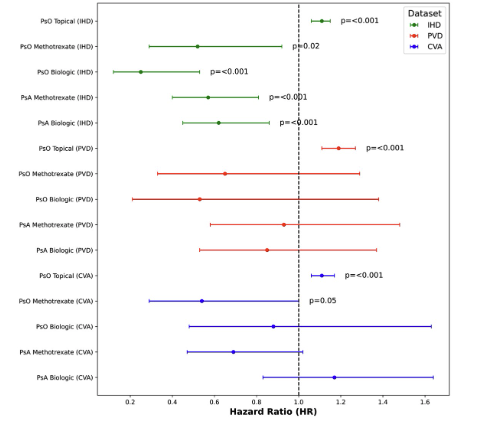
Ab#498 Does DMARD for PsO and PsA decrease MACE?
#ACR23 @RheumNow
Retrospective database Israeli study.
PsO, PsA on MTX or bDMARD: lower MACE compared to health matched controled (HR 0.45-0.68, p<0.001)
Pts on topical Rx had marginally Increased MACE (HR 1.14, p <0.001) https://t.co/0uRgjzYbFp
Eric Dein ( View Tweet)
Long term results of the MAINRITSAN study (Maintenance Remission w/ RTX in Systemic AAV) showed fixed-schedule RTX superior to AZA in preventing major relapses at 84mos (HR 0.38), but tailored-RTX assoc w/ incr risk of major relapse (HR 2.92) https://t.co/vucBYeM1P5 https://t.co/YqdqZWFhfd
Dr. John Cush RheumNow ( View Tweet)
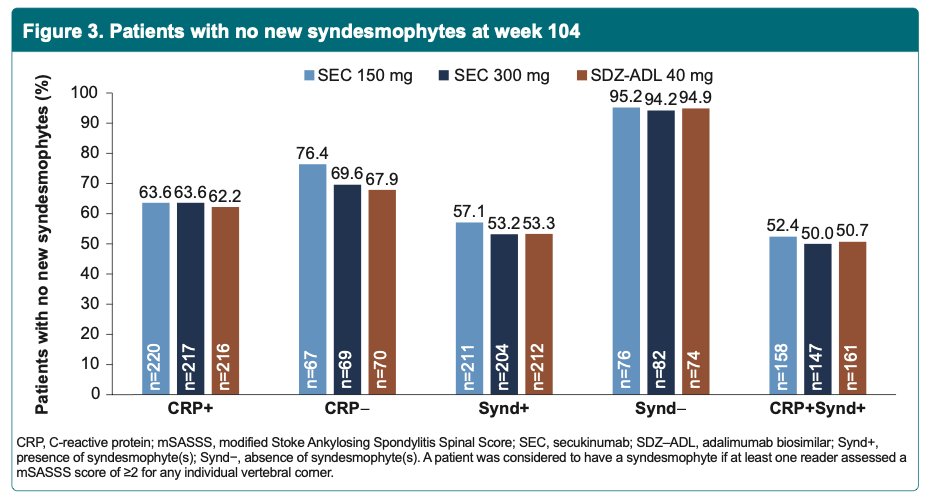
Is there a difference in secukinumab vs. adalimumab biosimilar on radiographic progression in a subgroup of axSpA pts with syndesmophytes or CRP levels?
Radiographic progression equally low in both drugs
NO difference in syndesmophytes or CRP
@RheumNow #ACR23 Abs#0522 https://t.co/1TBKAxuKPE
Robert B Chao, MD ( View Tweet)
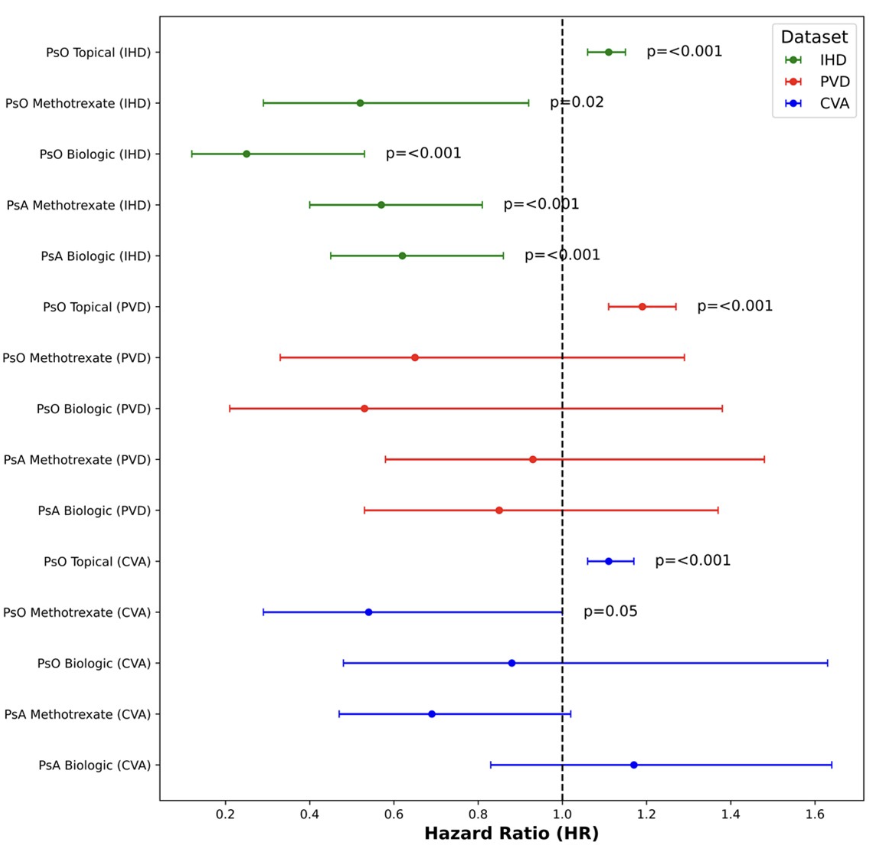
Systemic anti-inflammatory treatments for PsO and PsA including methotrexate and biologics provided cardioprotective effects
Potential cardiovascular benefits of IL-17i and IL-12/23i compared to TNFi
@RheumNow #ACR23 Abs#0498 https://t.co/Np7PSNvFd6
Robert B Chao, MD ( View Tweet)