All News

EULAR 2022 – Day 2 Report
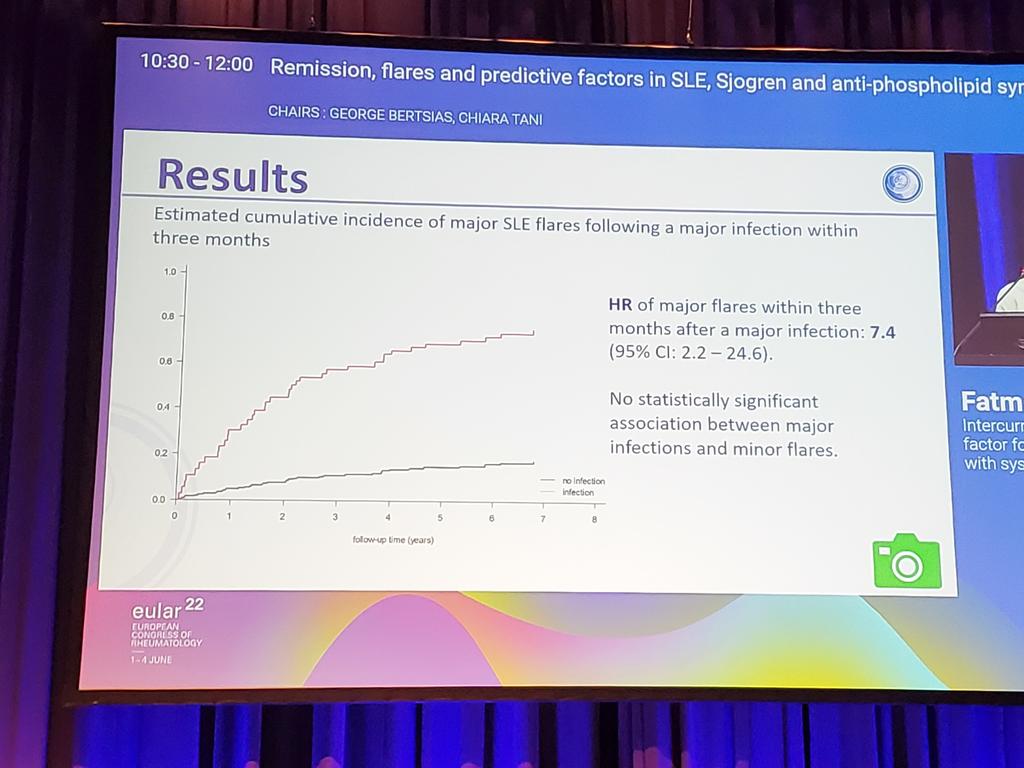
A full day at EULAR with oral and poster presentations of abstracts in the morning and a plethora of scientific (review) sessions in the afternoon. The latter covering topics like sarcoidosis, Still’s disease, fibromyalgia, back pain, sarcopenia, APS, IgG4 and imaging in vasculitis.
Read Article
Babies! Safety and Outcomes Data on Pregnancies
EULAR Congress 2022 highlighted several posters on pregnancy, an important subject as most rheumatic diseases afflicts women during their childbearing years.
Read Article
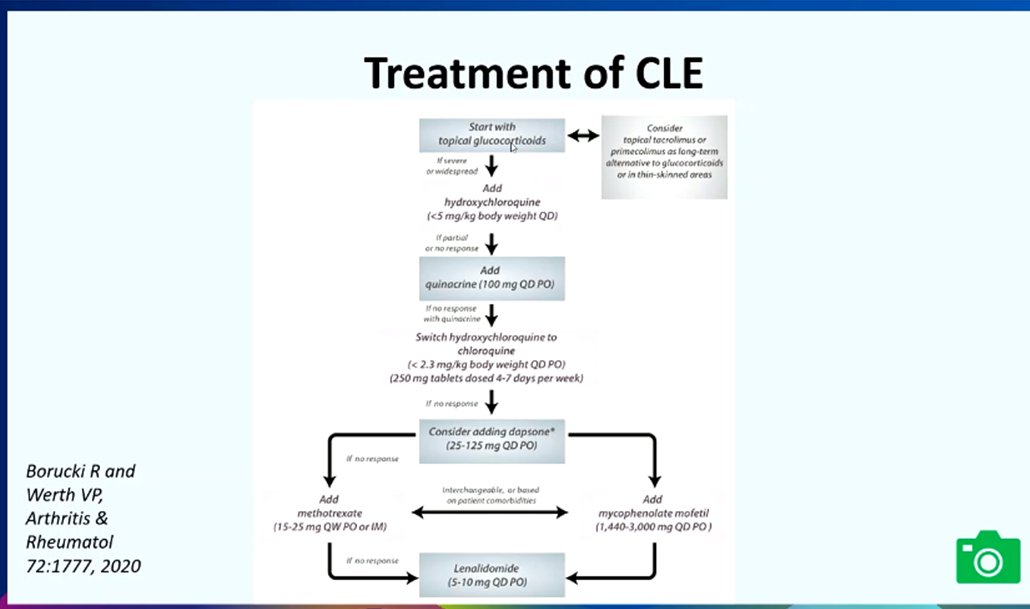
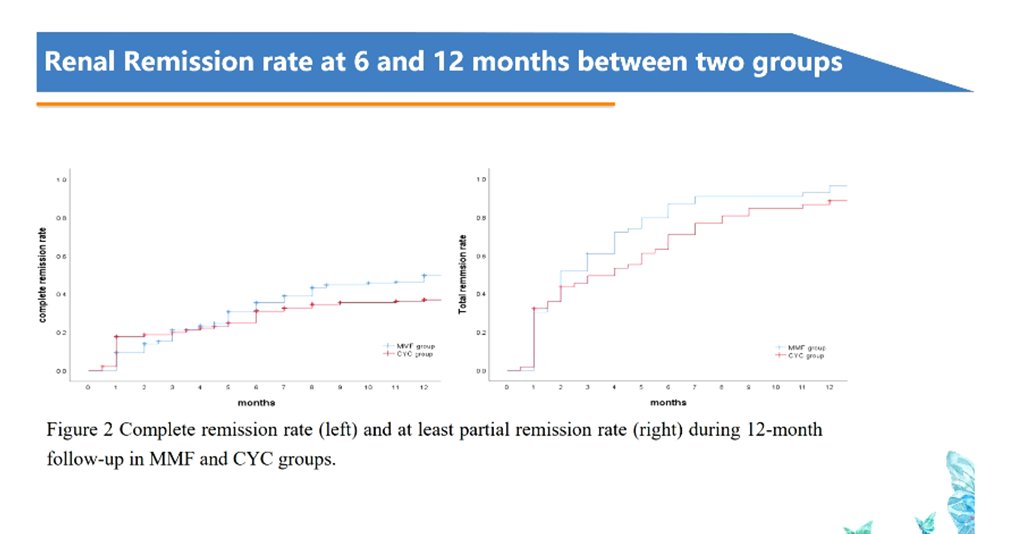
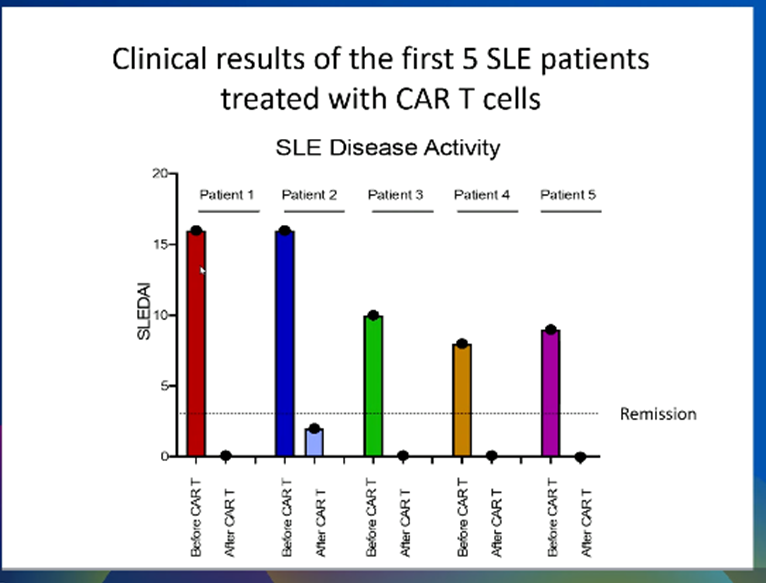
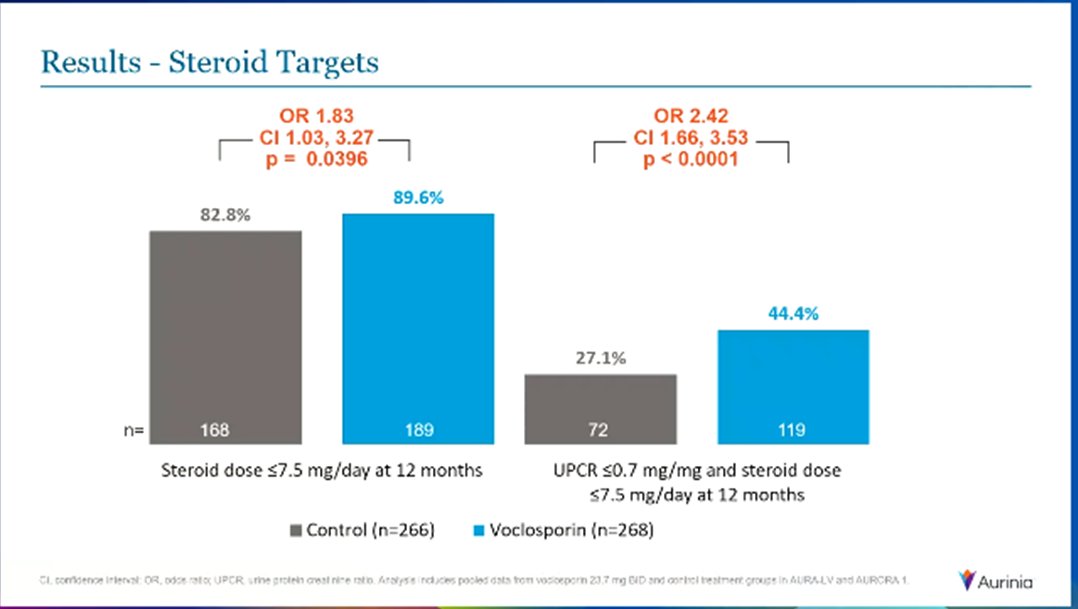
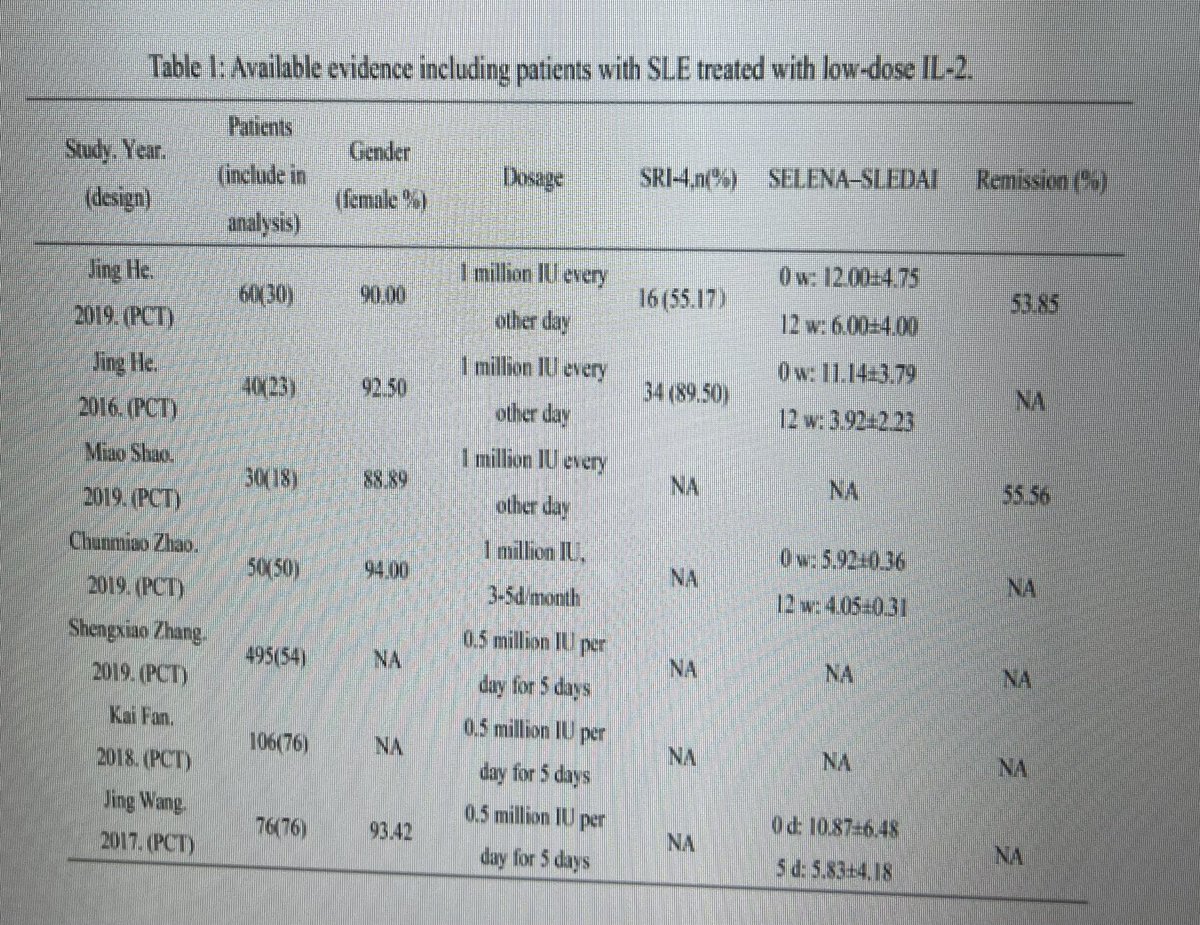
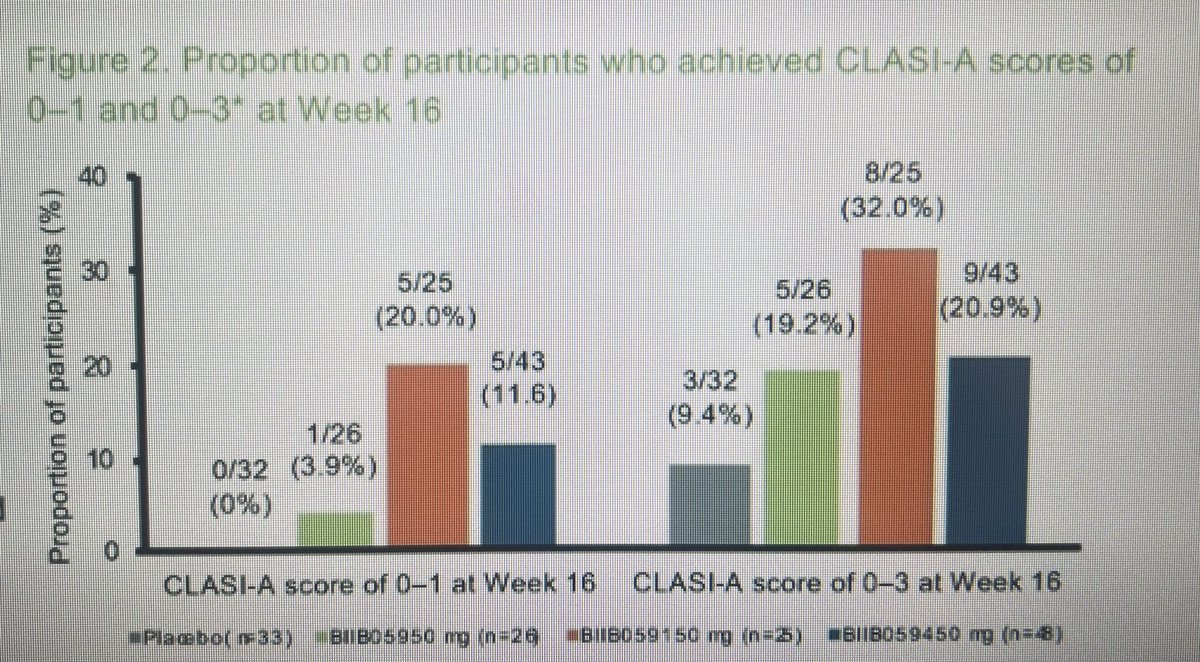
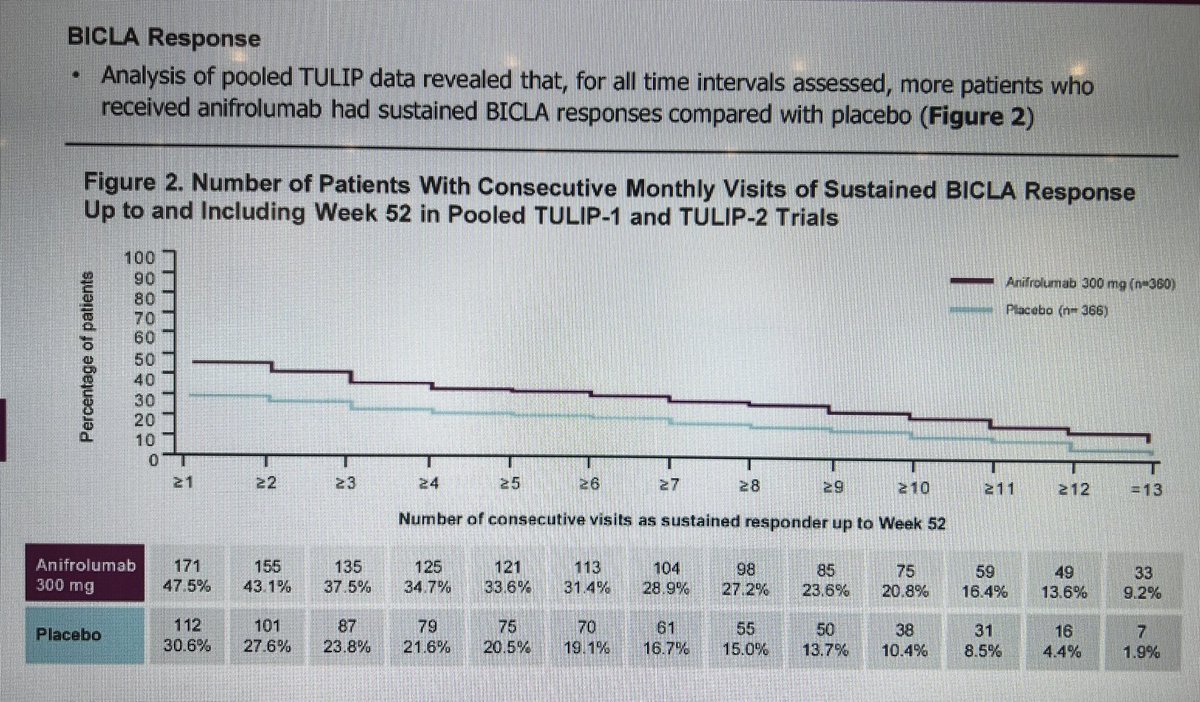
SLE trials update
Translating targeted therapy from bench to bedside has been more problematic in SLE than other autoimmune diseases, with many theoretically well-founded agents appearing to have failed in clinical trials as a result of inefficacy, problem with trial design and/or safety issues.
Read Article

TheDaoIndex KDAO2011 ( View Tweet)

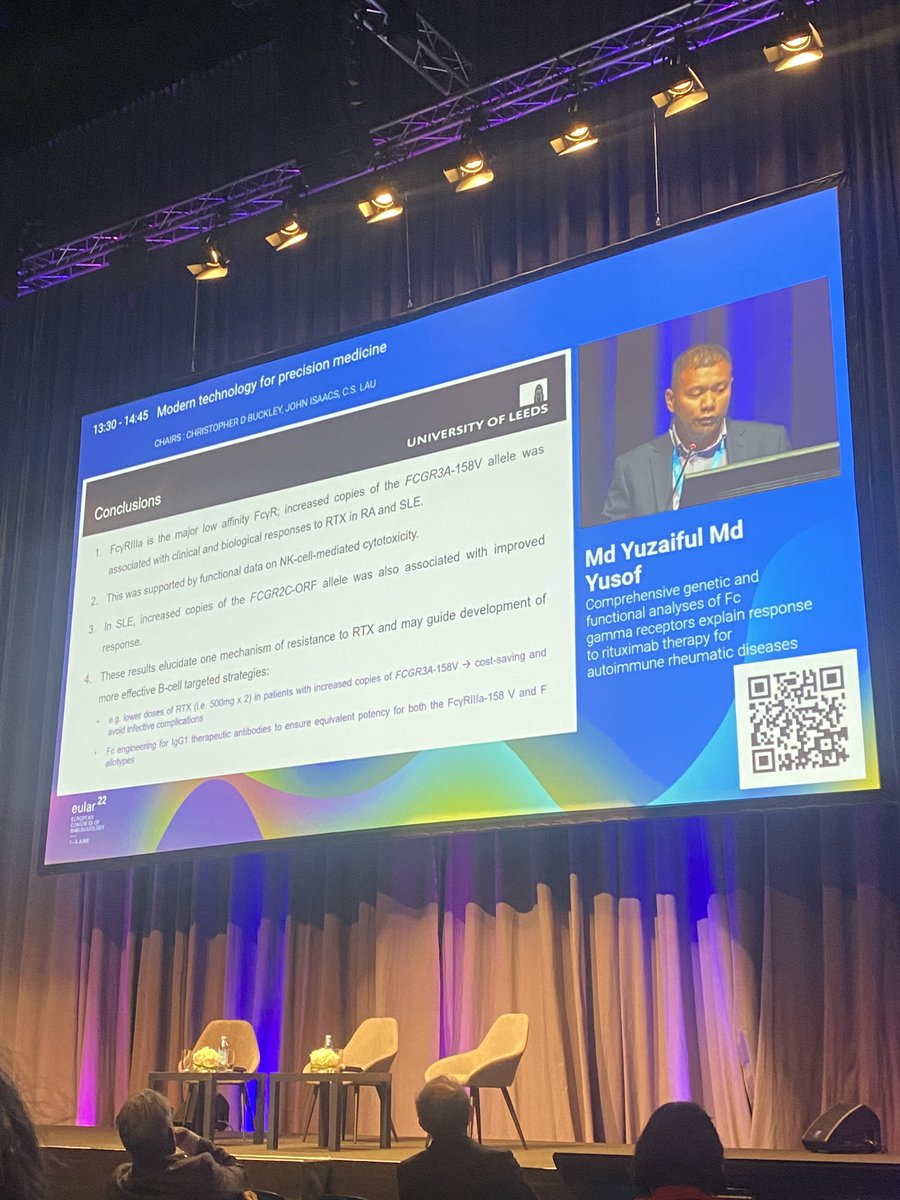
Md Yuzaiful Md Yusof Yuz6Yusof ( View Tweet)

Links:
TheDaoIndex KDAO2011 ( View Tweet)