
Articles By Md Yuzaiful Md Yusof, MRCP(UK), PhD

From BiTE to TriTE: Progress of T-cell Engagers in RMDs
The EULAR 2026 Congress in London showcased growing interest in T-cell engagers as a novel strategy to achieve deep B-cell depletion and drug-free remission in refractory rheumatic and musculoskeletal diseases (RMDs).
Read Article
5 years since Patient ID001: Progress on CAR-T Therapy in RMD
Five years on, are we closer to licensing of the first CAR-T therapy in rheumatic and musculoskeletal diseases (RMD)?
Read Article
Progress of biologics/targeted therapy in SLE
We are in a transformative era in SLE which generates excitement to both physicians and people living with lupus. We now have four licensed biologics/targeted therapies (i.e., belimumab, voclosporin and obinutuzumab for active lupus nephritis, and belimumab and anifrolumab for active non-renal SLE). Moreover, many other agents with different mode of action and administration are in late phase trials. This article previews some data being presented at EULAR 2026 Congress in London.
Read Article
Beyond malignancy, look out for LICATS with CAR-T
CAR T cell therapy took the centre stage in 2022 where data pertaining to a successful case series of 5 patients with refractory SLE were published by Prof Schett’s group. Since then, this area of therapeutic has expanded exponentially. Our growing enthusiasm was slightly dampened though when the FDA required all six approved CAR T-cell therapies in oncology to include a black box warning regarding the risk of second primary malignancies in January 2024. At ACR25, Prof Schett’s group described a new form of toxicity in patients with autoimmune disease receiving CAR T-cell therapy, most likely due to the cleansing of immune cells from the affected organs.
Read Article
Sjogren’s disease: two drugs with positive trials
After several failures of therapies in Phase 3 trials of Sjogren’s disease (SjD) over many years, all hope is not lost!
Read Article
SLE Conference Preview: progress in biologics
The pharmacology treatment including biologics, cellular-based therapies, and Bi-specific T-cell Engager (BiTE) in systemic lupus erythematosus (SLE) is a rapidly expanding field of research that provides excitement and optimism to both the patients and the physicians.
Read Article
ICYMI: SLE: advances to achieve deep B-cell depletion
The race is on for the first chimeric antigen receptor (CAR)-based therapy to be approved for the treatment of systemic lupus erythematosus. Its main principle is to induce deep B-cell depletion, with the hope to reset the B-cell aberrant immunity for a sustained clinical remission. At EULAR 2025 in Barcelona, several advances of CAR-based therapies will be presented.
Read Article
Promising role of Fc neonatal receptor blockade in autoimmune rheumatic diseases
During EULAR 2024, we learned about a novel mechanism of action therapy, nipocalimab in Sjogren’s disease (SjD). This is an anti-neonatal Fc receptor (FcRn) mAb that reduces circulating IgG, including autoantibodies, by selectively blocking the interaction of IgG with FcRn. A year on at EULAR 2025, data from Phase 2 RCT of efgartigimod, an FcRn-inhibitor were presented in autoantibodies positive, moderate to severe active SjD. In addition to SjD, data from Phase 2 RCT of efgartigimod in inflammatory myopathies was presented.
Read Article
Add-on certolizumab in pregnant women with APS
Women with antiphospholipid syndrome and lupus anti-coagulant are at high risk of developing adverse pregnancy outcomes (APO). Usual care includes low molecular weight heparin (LMWH) and low dose aspirin (LDA). Despite these therapies, APO have been reported up to 40%.
Read Article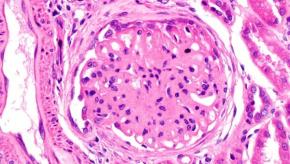
2025 update of EULAR recommendations on lupus nephritis
At the 2025 EULAR congress in Barcelona, Prof Dimitrios Boumpas presented a summary of the updated EULAR recommendations on the management of lupus nephritis (LN). The most significant change in the treatment paradigm of LN is that the historic standard of care (SOC) (i.e.
Read Article

