

Prevention in Lupus and Therapeutic Evolution in Sjögren’s Save

The notion of intervening in autoimmune disease prior to the onset of irreversible tissue damage has evolved beyond a theoretical framework; it is presently undergoing empirical evaluation. Recent discussions on incomplete lupus and the SMILE trial, alongside advances in Sjögren’s therapeutics, highlight both the promise and complexity of prevention and precision treatment in systemic autoimmunity.
Incomplete Lupus and the SMILE Trial
ANA positivity remains one of the most common referrals in rheumatology. As Nancy Olsen, MD, in her RheumNow Live 2026 lecture, SMILE Study - Hydroxychloroquine in ANA + Arthralgia, noted, 'at least 15%' of stacked referrals' at her institution were for ANA positivity. While '99% of lupus patients are ANA positive,' most positive ANA tests are not lupus. The clinical challenge lies in distinguishing benign autoimmunity from progressive disease.
Incomplete lupus—also referred to as latent lupus or preclinical autoimmunity—captures patients who are ANA-positive and meet one or two SLICC criteria but do not yet fulfill classification criteria for SLE.
Landmark longitudinal studies demonstrated that autoantibodies and cytokines accumulate years before clinical SLE. Cytokine elevations have been detected 'seven to eight years prior to their development of lupus,' suggesting a prolonged preclinical phase.
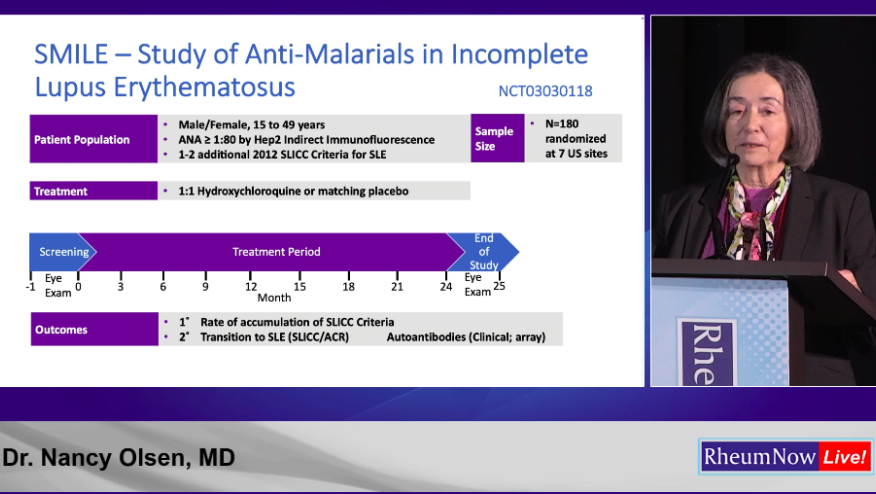
Hydroxychloroquine (HCQ) was selected for the SMILE (Study of Anti-Malarials in Incomplete Lupus Erythematosus) trial because it quenches the interferon signature and lowers BAFF levels in patients with incomplete SLE.
SMILE randomized ANA-positive patients aged 15–49 with one or two SLICC criteria to HCQ or placebo for 24 months. The primary endpoint was rate of accumulation SLICC criteria. Secondary endpoints were the transition to SLE and Autoantibodies. Ultimately, HCQ did not significantly reduce SLICC progression nor transition to SLE. However, HCQ did reduce IgG autoantibody levels across a broad antigen array but did not stop SLICC progression.
Sjögren’s: Precision Therapy on the Horizon![]()
![]()
In contrast to prevention in lupus, Sjögren’s research is focused on improving systemic disease activity in established disease. Matthew Baker, MD, from Stanford Medicine presented Sjogren’s Treatment Landscape in 2026. One challenge highlighted was that systemic disease activity scores and symptom scores 'do not correlate well,' meaning improvement in systemic inflammation does not always translate into patient outcme such as better dryness or fatigue.
Multiple prior trials of TNF inhibitors, IL-6 blockade, and abatacept were negative. However, newer B-cell–directed approaches show promise. As emphasized during the session, 'Targeting B cells is fundamentally a rational and probably effective approach.'
Phase 3 trials of BAFF receptor blockade, CD40–CD40L inhibition, FcRn inhibition, and dual BAFF/APRIL blockade have demonstrated statistically significant reductions in systemic disease activity. Post hoc analyses suggest patients with preserved salivary reserve may experience meaningful improvement in oral dryness, supporting earlier intervention.
Emerging concepts of 'endotypes'—biologically defined subtypes characterized by distinct pathophysiologic mechanisms—may allow for more precise therapeutic targeting in the future.
Key Takeaways
• ANA positivity is common, but progression risk is heterogeneous.
• SMILE did not prevent SLE progression but demonstrated biologic effects of HCQ.
• Lupus prevention likely requires targeting upstream inflammatory amplification.
• In Sjögren’s, B-cell–directed therapies are emerging as promising strategies.
• Precision medicine approaches using biologic endotypes may refine treatment selection.






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.