

Exciting Data for SLE: Plenaries from #ACR22 Save

ACR Convergence 2022 promises to be another exciting year for research in systemic lupus erythematosus (SLE), with multiple plenary sessions devoted to therapeutic advancements. Here’s a quick rundown of what to expect!
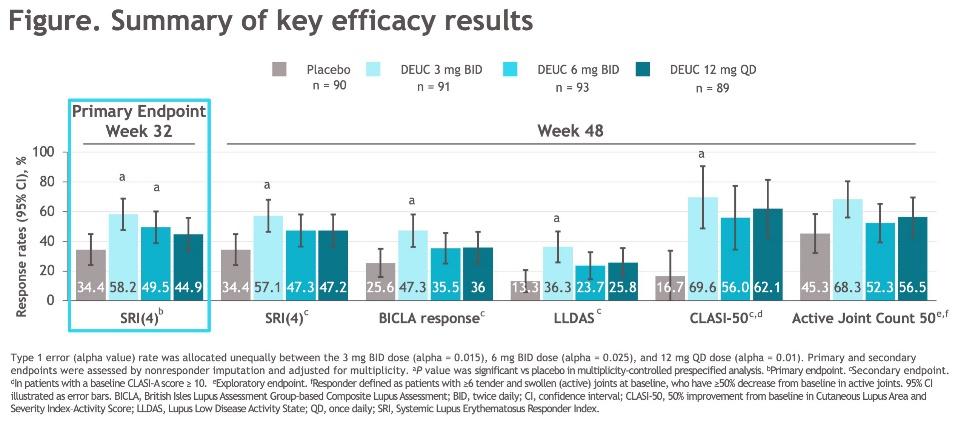
A new mechanism for SLE? The janus kinase (JAK) inhibitors have been an exciting pathway for rheumatology, but trials in SLE have been less encouraging and a development program for baricitinib was discontinued before phase 3 trials commenced. Yet hope springs eternal in SLE research and a plenary session (1117) on Sunday, November 13th at 11:45AM will share data about the tyrosine kinase 2 (TYK2) inhibitor deucravacitinib, which inhibits IL12, IL23, and IFNy. This large (363 patients!) phase 2 trial observed a significant improvement across multiple outcome measures and across multiple doses of deucravacitinib as opposed to placebo, including absolute improvement rates of 24% for SRI4 and 52% for CLASI-50. Could this be the best-yet of the recent biologic / targeted DMARDs in SLE? We’ll need Phase 3 data to be sure, but keep an eye on this space.
Lupus Adjacent: CART in APS? The recent publication of chimeric antigen receptor (CAR-T) therapy in a case series of 5 patients with SLE generated a lot of excitement. The idea behind CAR-T therapy is that we can genetically engineer T cells to go in and do our work for us. While this may bring about more durable B cell depletion, it could also be used to bring about more specific B cell depletion. In a plenary session on Monday, November 14th at 11:00AM, Max Konig will be presenting a potentially revolutionary study on antigen-specific CAR-T therapy for antiphospholipid antibody syndrome. Using CRISPR-Cas9, they successfully engineered T cells to specifically eliminated anti-beta 2 glycoprotein 1 expressing B cells. Were this to be successful when expanded, we could theoretically get all of the benefits of rituximab and other B cell depleting therapies with virtually none of the immunosuppression. Though it is still early in the development, it would be a true “holy grail” were it to be successful at scale and in human trials with clinical outcomes.
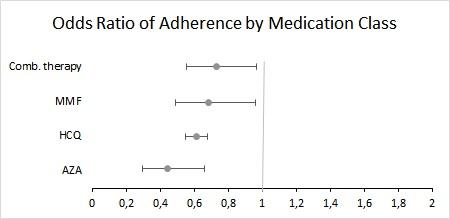
Cheaper Alternatives: Stop Charging People: The third plenary that really caught my eye involved a large claims database and copays for common medications for SLE. It will be presented on Sunday November 13th by Raisa Lomanto it describes the association between copays and adherence to hydroxychloroquine, azathioprine, and mycophenolate. Somewhat unsurprisingly, they found significant relationships for all three drugs, suggesting that charging a copay lowers adherence. What I did find notable was the magnitude of the effect; copays lowered adherence to hydroxychloroquine by 39%, azathioprine by 56%, and mycophenolate by 32%. For the cost of a single year of deucravacitinib ($75,000 per year), we could cover copays (median price $7 to $10) for all three drugs for 2,500 patients with SLE. Always remember to keep public policy in mind!






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.