News

CAR-T Therapy: EULAR 2026 Conference Recap
CAR-T therapy in autoimmune disease is moving fast - but is it ready to move beyond specialized referral centers? This EULAR 2026 recap covers the mechanistic data, relapse biology, and access innovations shaping that answer.
FDA Delays Gout Drug NASP with Complete Response Letter
At the end of June, Sobi was awaiting an FDA decision on its Biologics License Application (BLA) for NASP (nanoencapsulated sirolimus plus pegadricase) for the treatment of adult patients with uncontrolled gout. On June 26, 2026, SOBI received a Complete Response Letter from the U.S. FDA that will delay a decision on NASP, pending the company's answer to questions regarding the drugs manufacturing at a 3rd party facility in China.
Problems with treatment adherence in the management of gout
Compared to common medical conditions such as hypertension, type 2 diabetes, hyperlipidemia or osteoporosis, where the reported drug adherence rates are between 50% to 70%, the drug adherence for gout is 37%.
NEJM Retracts Pivotal ADVOCATE Trial of FDA-Approved Avacopan
MedPage Today
The New England Journal of Medicine (NEJM) retracted the pivotal study supporting FDA's approval of avacopan (Tavneos) for severe forms of anti-neutrophil cytoplasmic

DMARD Efficacy in RA-ILD
A network meta-analysis in the Journal of Autoimmunity reviews the pharmacologic options for rheumatoid arthritis–associated interstitial lung disease (RA-ILD). RA-ILD guidelines were recently presented by ERS/EULAR, but these were mainly conditional, low-certainty recommendations.
The Power of Self-Management with Chronic Low Back Pain
EurekAlert!
Almost everyone will deal with back pain at some point in their lives.
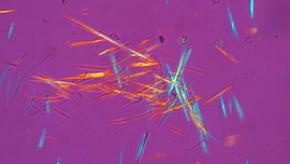
Uric Acid: Is Lower Better?
Lowering serum urate and urate crystals in the body is indispensable for long-term management of gout. The pathophysiology is simple and powerful: no urate crystals, no gout flares.

ICYMI: Updated CRA/SPARCC Recommendations for Axial Spondyloarthritis
In 2024, the Canadian Rheumatology Association (CMA) and the Spondyloarthritis Research Consortium of Canada (SPARCC) published a comprehensive set of 56 treatment recommendations for the management of axial spondyloarthritis. This first update is focused on the reassessment of IL-17i recommendations.
EULAR26: ANCHOR-RA Study of RA-ILD
EurekAlert!
People with rheumatoid arthritis are at risk of developing interstitial lung disease (RA-ILD), which is associated with high mortality.
EULAR26: Vasculitis updates: Glucorticoid use in AAV and GCA
EurekAlert!