All News

The Need for Comparative Treatment Trials in Psoriatic Arthritis
Psoriatic arthritis is currently experiencing a burgeoning selection of treatment options. While this is a very welcome development in a disease which has had less treatment options compared to RA, it leaves us with a difficult conundrum: which agent to choose for an individual patient.
Read Article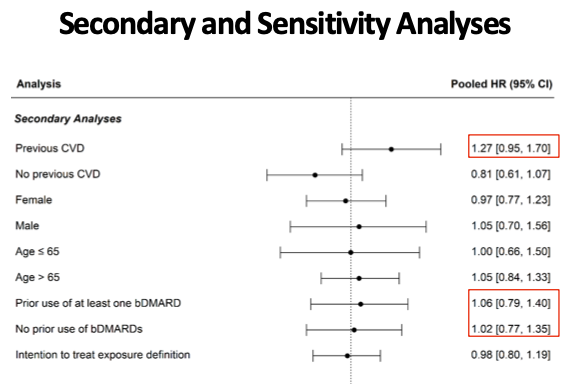
#ACR21 Ab#1939: Tofa CV Outcome (STAR-RA)
▶️Pooled data does not show ⬆️ risk of CVD
▶️Trend in pts w prior CVD -HR 1.27 (0.95-1.7), cannot r/o CVD risk in pts w risk factors
Less clear than oral surveillance data, but concerns in those w risks
https://t.co/JOKNyYVZfX @Rheumnow https://t.co/GGYJfxcqhc
Links:
Eric Dein ericdeinmd ( View Tweet)
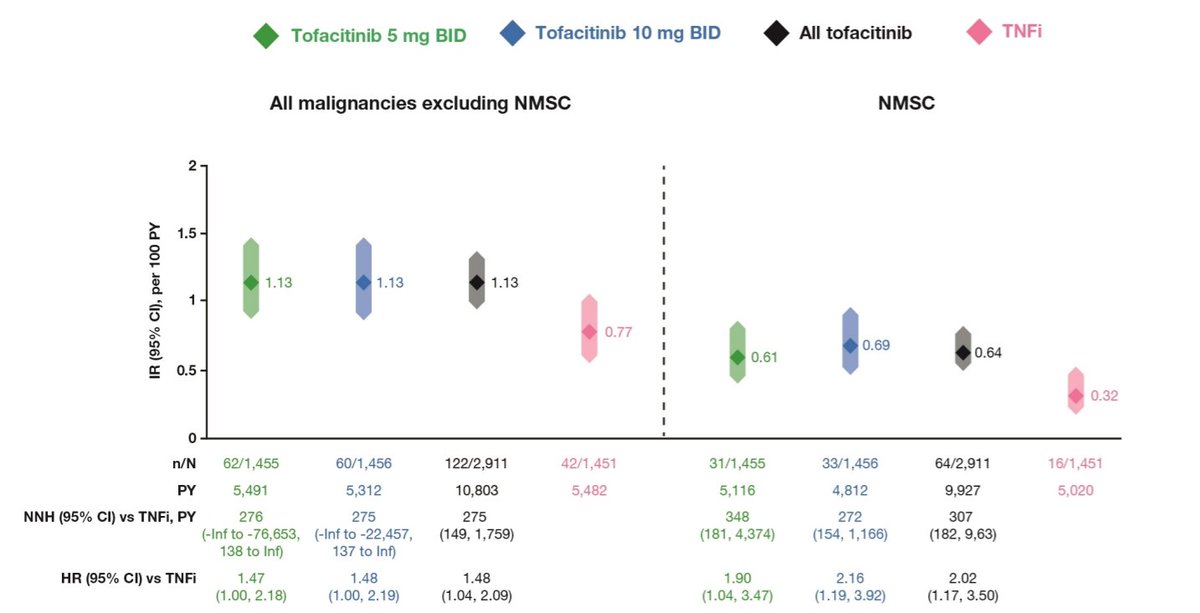
ORAL Surveillance malignancy risk @RADoctor . Numerically higher at both doses tofacitinib compared to TNFi . Abstr#1940 #ACR21 @RheumNow https://t.co/uc2k5EaiRq
Richard Conway RichardPAConway ( View Tweet)
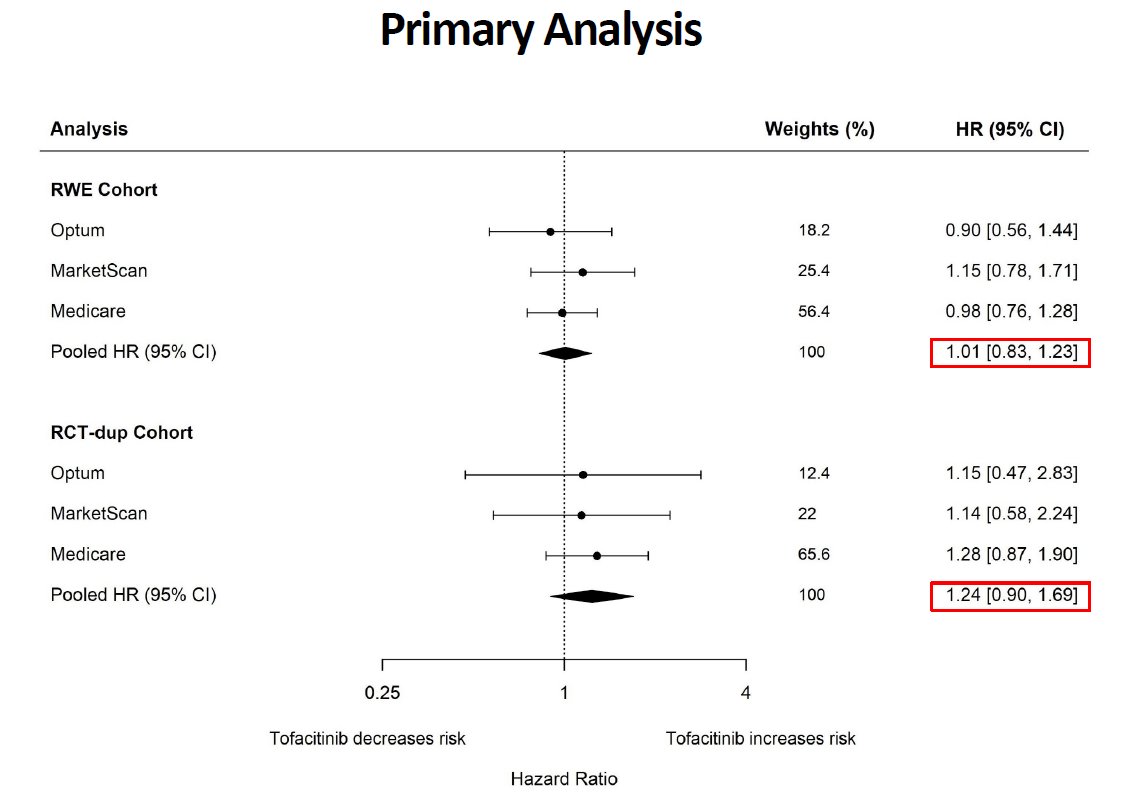
STAR-RA, CV risk
large insurance datax3
tofa vs TNFi
all comers: HR 1.01 (0.83-1.23)
one CV RF + any MTX: HR 1.24 (0.90-1.69)
prev CVD: HR 1.27 (0.95-1.70)
not sig
but surely okay to say baseline CV risk + tofa makes me a little nervous?
@SeoyoungCKim #ACR21 ABST1939 @RheumNow https://t.co/LmmL5zgv9u
David Liew drdavidliew ( View Tweet)
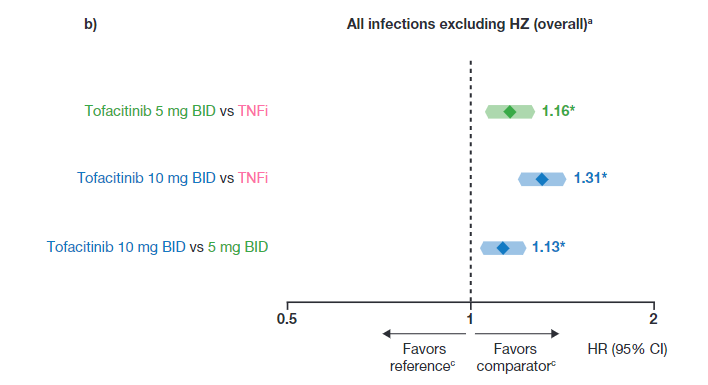
ORAL Surveillance: MACE and malignancy are getting all the attention...
but did you know that non-zoster infections are also more likely with tofacitinib vs TNFis?
#ACR21 ABST1684 @RheumNow https://t.co/GiBkvPYs4j
David Liew drdavidliew ( View Tweet)
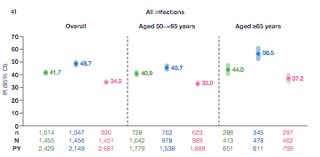
Serious infections beyond herpes zoster in both doses of #tofacitinib v #TNFi in Oral Surveillance. Note this outcome was not powered to be stat sig. it is a comparison of SIE events #ACR21 abst#1684 @RheumNow https://t.co/uqME6ABXuC
Janet Pope Janetbirdope ( View Tweet)
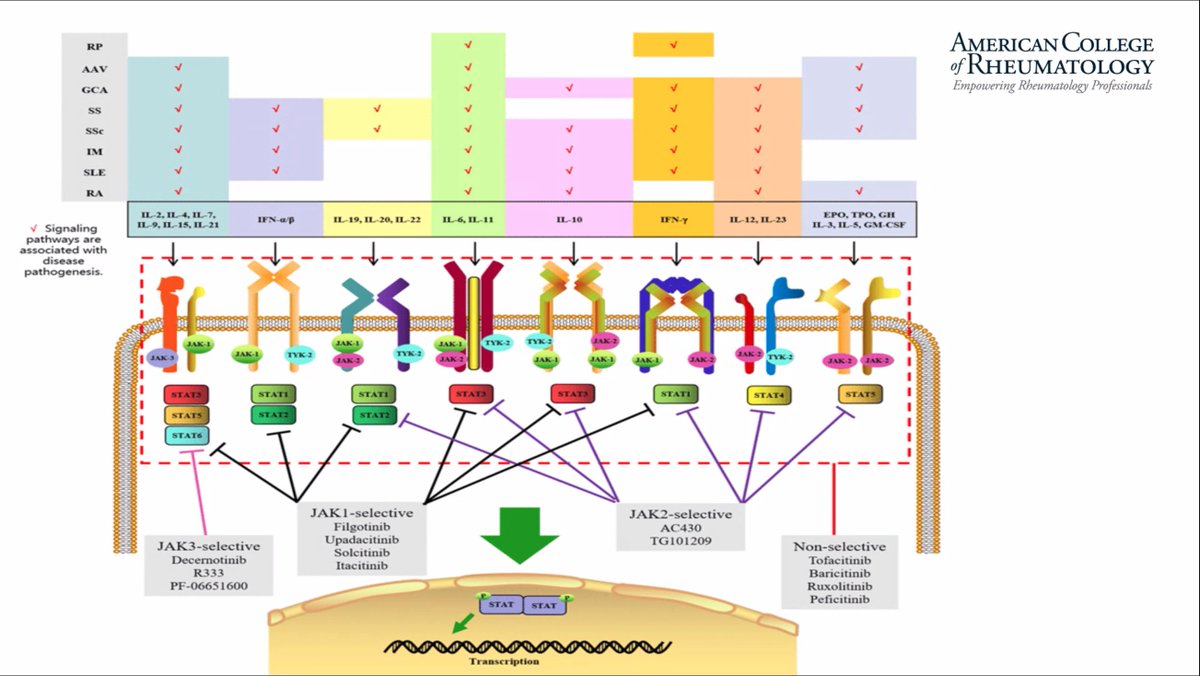
Handy overview of Jak/STAT pathways in rheumatic diseases and available inhibitors (Dr. Joost Swart). Happening now in the Pediatrics Hub (New Therapies & Biologic Safety in Pediatric Rheumatology). #ACR21 #pedsrheum https://t.co/i4bYr4GKOP
Katie Poholek kpoho ( View Tweet)
Deucravacitinib is a novel, oral, selective TYK2 inhibitor in PsA and selectively mediates specific inflammatory pathways (IL-23, IL-12, Type I IFN). Listen to my interview with Prof. Oliver Fitzgerald on this and his highlights https://t.co/3UJCwbHsLC
@RheumNow #ACR21 Abst#490 https://t.co/OWZDHhcQ9q
Dr. Antoni Chan synovialjoints ( View Tweet)
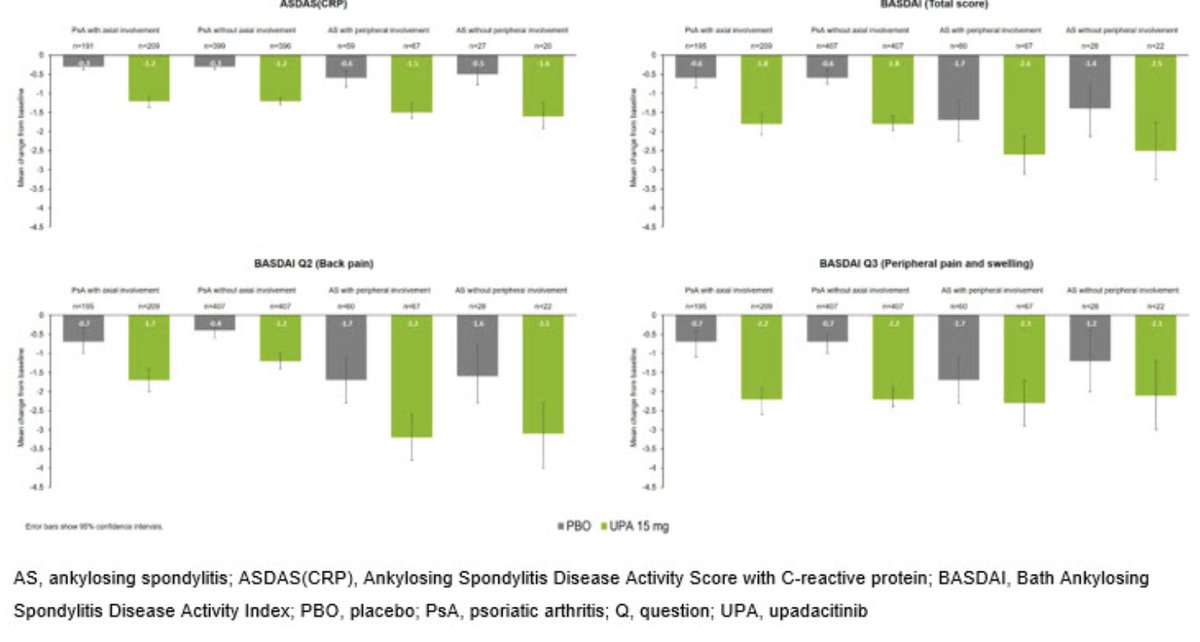
Upadacitinib showed similar efficacy in AS pts compared to PsA pts with axial involvement
⭐️PsA pt w/ axial involvement and AS pts with differences in baseline characteristics
#ACR21 @RheumNow
Abs#1802
https://t.co/QvyayelBYU https://t.co/50dNQm30vf
Links:
Robert B Chao, MD doctorRBC ( View Tweet)
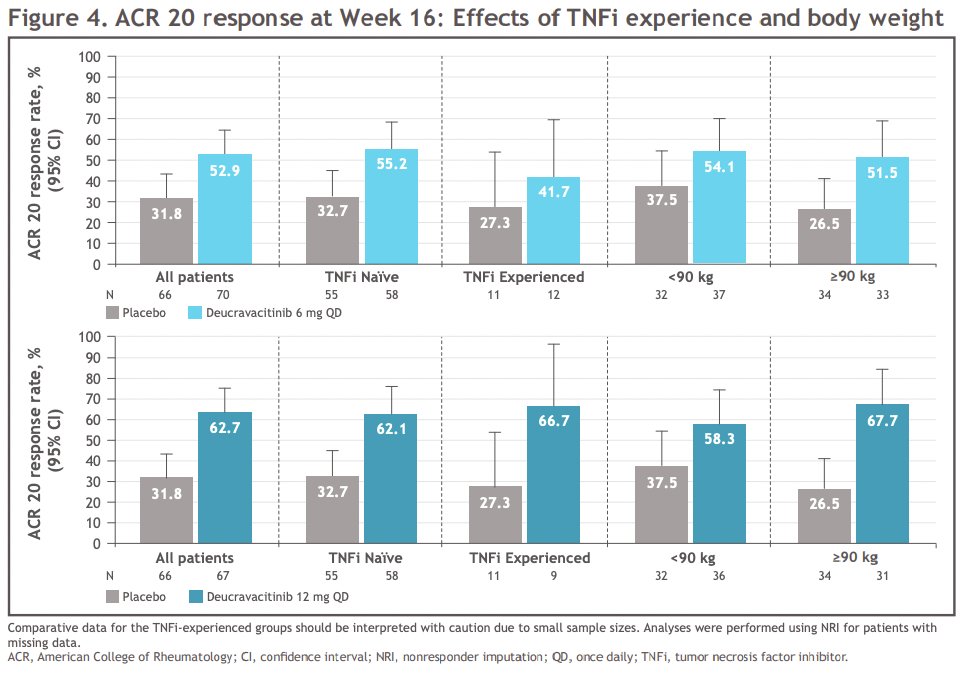
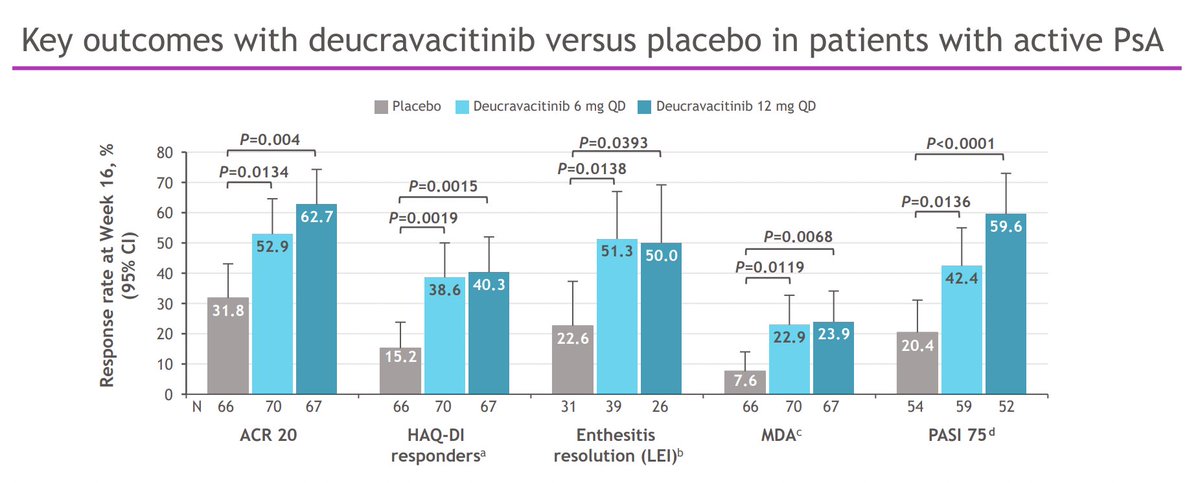
Phase 2 Placebo/Deucravacitinib 6mg/12mg od study ACR20 at 16 weeks of 31.8%/52.9%/62.7% respectively. Efficacy observed across TNFi and body weight subgroups. Safety profile similar to Phase 3 trials in patients with psoriasis @RheumNow #ACR21 Abst#1820 https://t.co/bOfEZdqN5Z https://t.co/EjMwWISM80
Dr. Antoni Chan synovialjoints ( View Tweet)
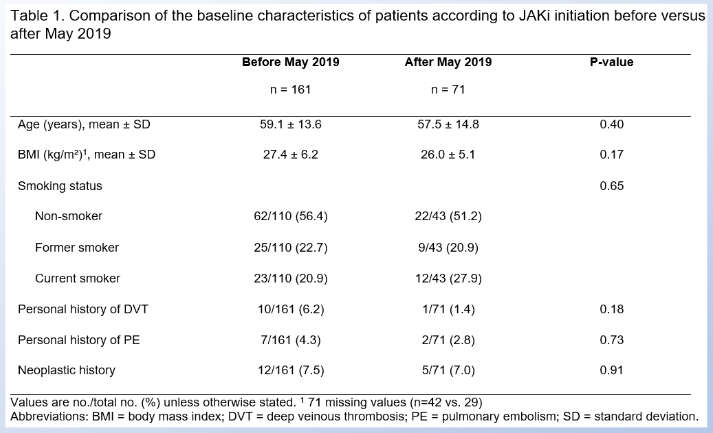
Will a FDA black box warning change your JAKi practice?
In May 2019, the EMA put out a warning about VTE with tofacitinib.
In this French cohort, did it change the kind of pts they initiated on JAKi?
no, not it did not😊
A window into the US future?
#ACR21 ABST1245 @RheumNow https://t.co/QI95E1gepg
David Liew drdavidliew ( View Tweet)
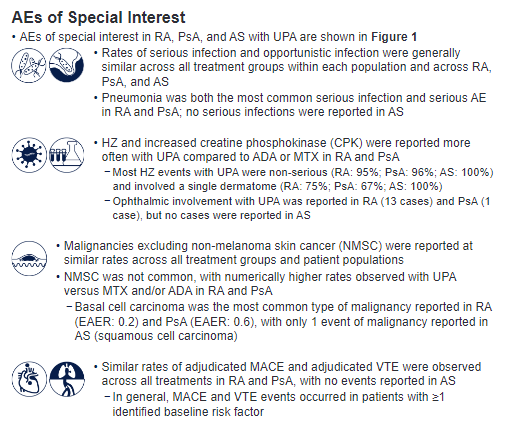
Safety profile of #upadacitinib in #RA, #PsA, #AnkylosingSpondylitis
👉🏼AE rates similar across UPA, ADA & MTX in RA, and UPA & ADA in PsA
👉🏼No new safety risks with long-term use
👉🏼#Herpeszoster & incr CPK more common w/ UPA vs ADA/MTX
Abs#1691 #ACR21 @RheumNow https://t.co/tKYi65kB5r
Mrinalini Dey DrMiniDey ( View Tweet)

ACR21 Best Abstracts We Saw - Day 3 (Monday)
The third day of ACR 2021 took a big leap in online content. Here is a compilation (with links) of presentations were the “ACRBest” as seen by our RheumNow faculty.
Read Article
Upadacitinib 56-wk efficacy/safety (mod to severe PsA)
🔹Comparable or ⬆️efficacy vs adalimumab
🔹Efficacy maintained, and 15mg vs 30mg doses similar at 56wks
🔹No new safety findings @ 56wks
🔹🚫inc risk VTE, MACE, cancer vs ada
https://t.co/NlKvBrwDxB
#ACR21 Abst#1345 @RheumNow
Pedro Castillo _Castillo_Pedro ( View Tweet)

Interesting question came up: why would you change a RA patient from JAKi to JAKi?
The main reason I can think of would be if the first JAKi worked a bit (but not enough to continue, or AEs got in the way).
That would clearly favour to better survival
#ACR21 ABST1442 @RheumNow https://t.co/kDiJVbJfit
David Liew drdavidliew ( View Tweet)
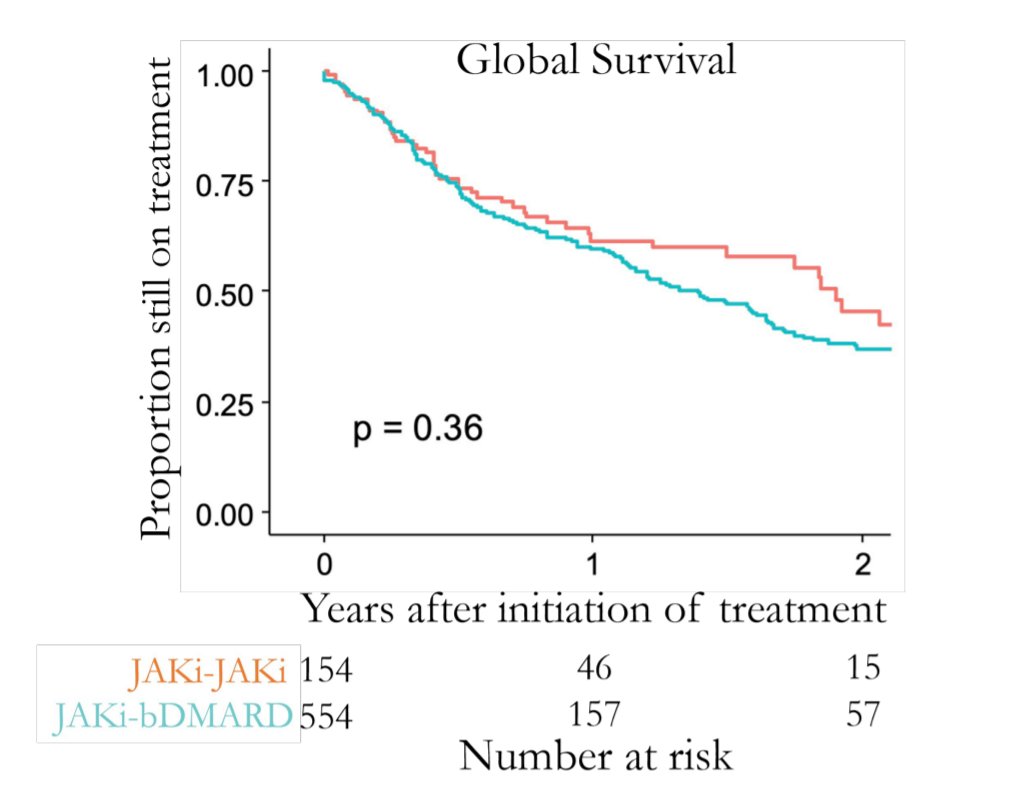
JAK-pot registry-based study. Following JAKi failure should you switch mode of action or go to second JAKi? Both seem equally effective in terms of drug retention. Didn't matter if switch for efficacy or adverse event. Abstr#1442 #ACR21 @RheumNow https://t.co/QEBB3flArC
Richard Conway RichardPAConway ( View Tweet)
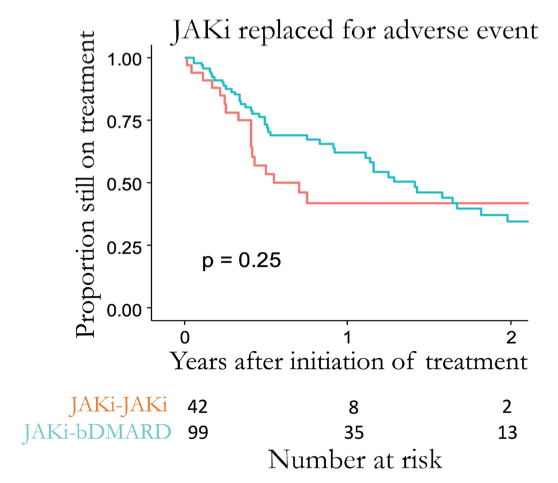
#ACR21 Abs#1442: JAKpot - Cycle JAK or switch to bDMARD after JAK failure?
▶️No difference between cycle vs bDMARD group
▶️Non-signif trends: cycled JAK better for inefficacy to 1st JAK, bDMARD better for adverse effects
@Rheumnow https://t.co/6UNUVh5ZW8 https://t.co/upfI6tDH1p
Links:
Eric Dein ericdeinmd ( View Tweet)
First JAKi failure: What's next? Wanna find out? It's here
https://t.co/o5CE1MBzUu
Abstr#1442 #ACR21 @RheumNow https://t.co/f0sdPn5mcZ
Aurelie Najm AurelieRheumo ( View Tweet)

⭐️ Wanna catch up with the latest news on JAKi safety trials presented at #ACR21? Our @Rheumnow interview with @ErnestChoy1 is out. Link below
https://t.co/zYb4rXcw1x https://t.co/i39xXnfC3Q
Aurelie Najm AurelieRheumo ( View Tweet)
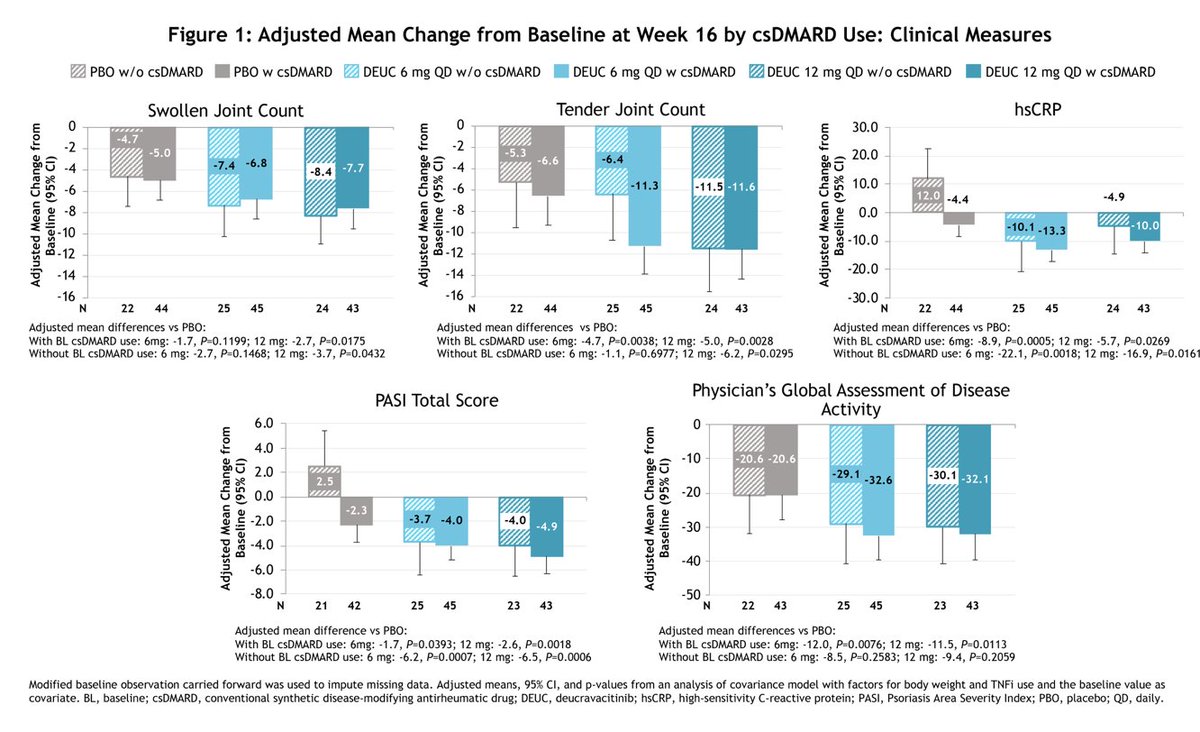
Post-hoc analysis of Deucravacitinib (TYK2i) for tx of PsA showed similar efficacy in pts with and without background csDMARD use.
⭐️>60% w/ background csDMARD use, majority of which was MTX
⭐️no difference in AE
#ACR21
Abs#1352
@RheumNow
https://t.co/nIJT7rNkJP https://t.co/bq0x1Ywguo
Robert B Chao, MD doctorRBC ( View Tweet)