

Statin-Induced Autoimmune Myopathy Save

The CDC estimates nearly 71% of adults with cardiovascular disease and 54% of adults with hypercholesterolemia use a cholesterol-lowering
medication, and that "statin" use has grown significantly in recent years. During 2003–2012, statin use has increased from 20% to 28% in adults over age 40 years.
Statins significantly reduce the incidence of cardiovascular disease, and generally have an acceptable side-effect profile. Myalgias are not uncommon but myopathy occurs in less than 1% and rhabdomyolysis is very rare.
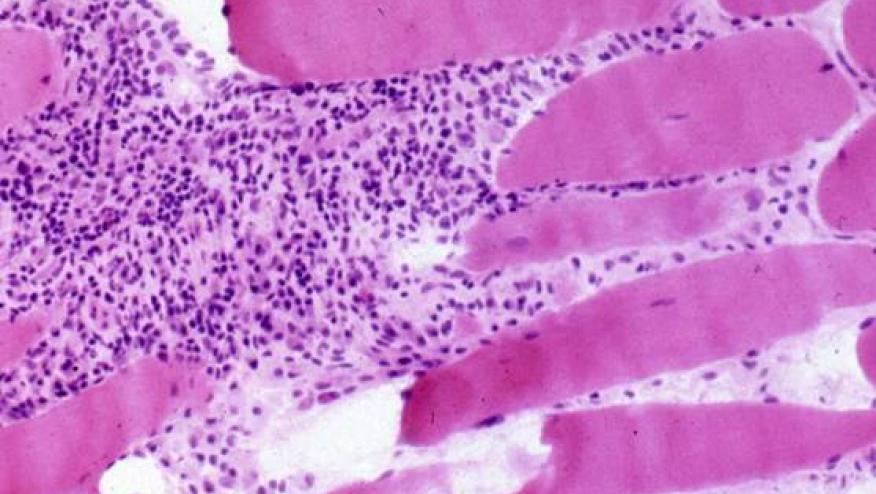
There are, however, reports of autoimmune myopathy directly related to statins. These usually have symptomatic weakness, evidence of necrotizing myositis on biopsy, and autoantibodies against 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase. This syndrome of statin-associated was recently reviewed in the Feb. 18th issue of the New England Journal.
The syndrome is exceptionally rare and is estimated to occur in approximately 2 or 3 of every 100,000 patients treated with statins. The onset need not be after initiation and may occur after years of statin therapy. Myalgia, mild-to-moderate weakness are occasionally accompanied by joint pains or a rash. A myopathy should be suspected when finding elevated creatine kinase levels (usally > 2000 IU/L). Electromyography shows small-amplitude motor-unit potentials with increased spontaneous activity characteristic of an active myopathic process, and muscle edema is evident on magnetic resonance imaging (MRI).
The diagnosis may be confirmed by serologic testing for HMG-CoA reductase antibodies. While not widely available they can be assayed in a few laboratories including RDL reference lab in California. One study found that 24 of 26 patients (92%) who were positive for anti–HMG-CoA reductase autoantibodies and were older than 50 years of age had taken statins before the onset of the disease. While such antibodies are not found in patients without disease (and on statins), up to 1/3 of patients anti–HMG-CoA reductase antibodies may not have a history of statin exposure. Such patients are younger and may have a less responsive form of myopathy.
Treatment begins with discontinuation of the statin, as this results in improvement in some. Otherwise, those with more severe or persistent myositis should be treated with the same glucocorticoid and immunosuppressive regimens used to manage polymyositis, including the use of methotrexate, azathioprine, mycophenolate mofetil, intravenous immune globulin or rituximab. Greater than half of patients will need aggressive therapy.
Once recognized and treated, most patients have favorable outcomes and the return of muscle strenght.
Continue Reading
Join The Discussion
What is your experience with Zetia as cause of Myalgias?
I explored this literature a few times and it seems it has been reported but infrequent. It has come up occasionally in a few patients I have seen.-thanks!
Disclosures
The author has no conflicts of interest to disclose related to this subject






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.