

ACR22: Polymyalgia Rheumatica in the Spotlight Save

One of the enduring legacies of ACR 2022 for me will be the emphasis on polymyalgia rheumatica (PMR). Despite being highly inflammatory and relatively common, a remarkable paucity of trials have been run in this space. Read on for a quick PMR-roundup from the meeting!
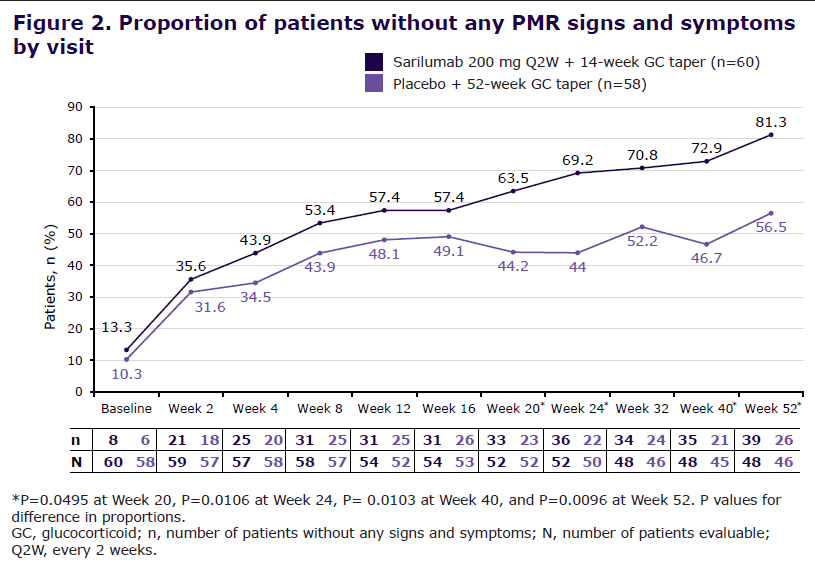
The highlight for me was the SAPHYR study (Abstract 1676), which evaluated the IL-6 inhibitor sarilumab among patients with relapsing polymyalgia rheumatic in a phase 3 double blind randomized controlled trial. In the study, 118 patients were randomized to receive sarilumab 200mg every 2 weeks and a 14 week glucocorticoid taper or placebo and a 52 week glucocorticoid taper. The trial was ultimately successful, with number needed to treat to obtain sustained remission of roughly 5 patients.
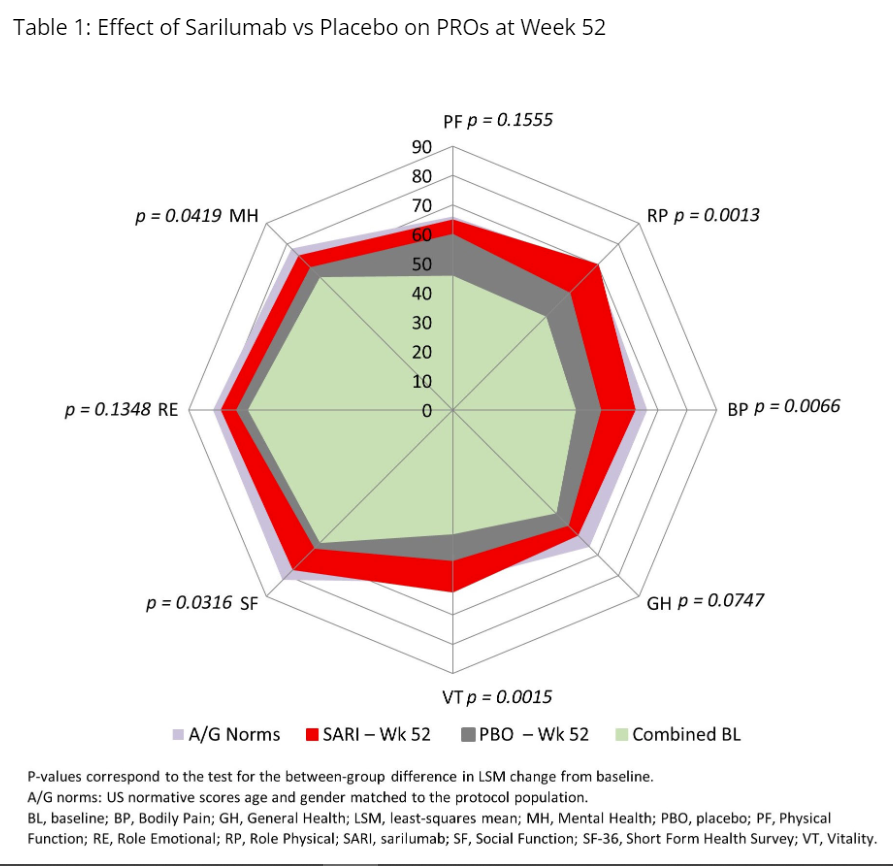
This alone would have been exciting, but flares in PMR can be quite mild, merely requiring a return to a previous dose or a small increase in the daily dose of glucocorticoids. As a practicing rheumatologist, what I really care about is whether my patients live longer or live better because of the therapy I offer. In the SAPHYR study, patient reported outcome measures (PROs) also favored the treatment arm (Abstract 2243). Differences were not only statistically significant, but also met minimally clinically important differences.
In addition to sarilumab, abstract 1106 evaluated the IL6 inhibitor tocilizumab. Similar findings were observed, with a 36% reduction in the primary endpoint of a PMR activity score that included the CRP. I had never heard of this outcome measure and – unlike the aforementioned SF-36 – it does not have a defined minimally clinically important difference. That said, patients randomized to tocilizumab were also more likely to be flare free and more likely to be able to reduce or discontinue prednisone. Though the trial itself was smaller and may not be sufficient for FDA approval, it provides additional support for the IL-6 pathway in PMR.
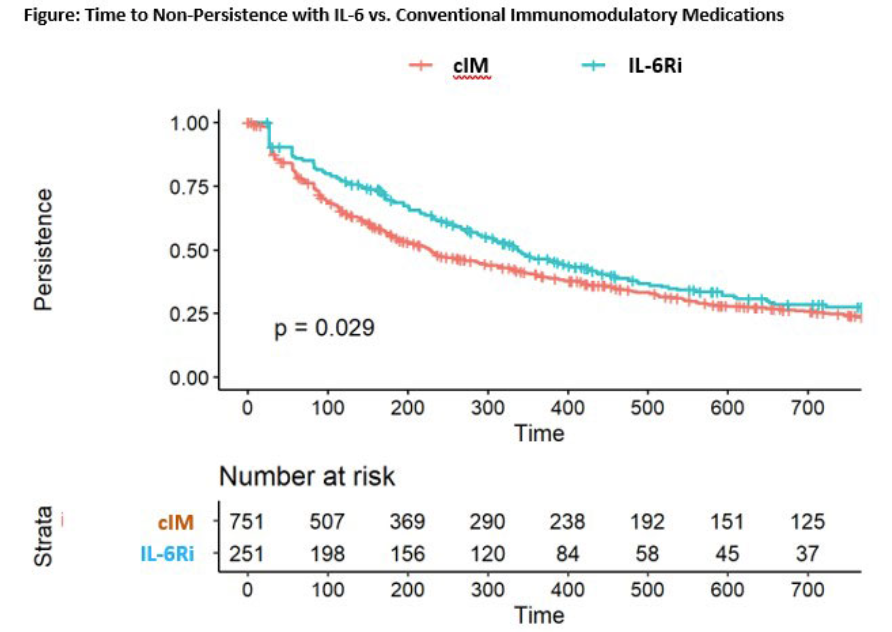
Typically we need to wait for FDA approval to find out whether clinical trial data will apply in the “real world,” but Abstract 1547 somewhat serendipitously arrived during ACR 2022 as well. In this “real world” dataset using a Medicare data sample, 409 “3rd line” and 251 “2nd line” patients who received IL-6 inhibitors or conventional immunotherapies were identified. Those who received IL-6 inhibitors – as opposed to conventional immunotherapies – were significantly more likely to stop glucocorticoids over time.
Ultimately, we will have to await additional studies and regulatory approval before this will be readily available. It seems unlikely that I would use either agent in all patients, but will likely restrict to relapsing and refractory patients. My ultimate hope, though, is that PMR goes the way of GCA after the GiACTA trial, where early success in the IL6 pathway created an explosion of interest in the disease and the initiation of multiple clinical trials with different mechanisms.






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.