

FAST, FREED, CARES, & CONFIRMS: A Run-Down on the Black-Box Blues of Febuxostat Save


Febuxostat, a nonpurine xanthine oxidase inhibitor used in the treatment of chronic gout to lower serum urate levels, received bad press in 2019 after the US Food and Drug Administration (FDA) placed a black-box warning on the medication’s label suggesting that it increases the risk of cardiovascular (CV) death in patients with preexisting CV disease. This was met with disappointment by many Rheumatologists and has remained a topic of controversy with many healthcare providers avoiding prescribing febuxostat in patients with CV disease. This controversy merits a review of the literature, especially in light of an exciting, late-breaking addition to the evidence, the FAST trial (revealed on November 9, 2020), that seemingly puts the controversy to rest.
The CONFIRMS trial in 2010 published in Arthritis Research Therapy by Becker et al was a multicenter, phase III, double-blind, randomized control trial that showed that the urate-lowering efficacy of febuxostat 80 mg exceeded that of febuxostat 40 mg and allopurinol 300 mg (200 mg in renal impairment) in 2,269 patients with gout and serum urate (sUA) > or = 8.0 mg/dL. It also showed that either febuxostat dose was more efficacious than allopurinol. Most importantly, it showed that the safety of febuxostat and allopurinol was comparable. Specifically, blinded adjudicated CV event rates were 0.0% for febuxostat 40 mg and 0.4% for both febuxostat 80 mg and allopurinol. Notably, co-morbidities of the study population included renal impairment (65%), obesity (64%), hyperlipidemia (42%), and hypertension (53%).
The CARES trial in 2018 published in the NEJM by White et al was a multicenter, double-blind, non-inferiority trial involving patients with gout and CV disease that assigned 6,190 gout patients to receive febuxostat (median 728 days) or allopurinol (median 719 days). Notably, the trial regimen was discontinued in ~57% of patients and 45% of patients discontinued follow-up. The median duration of follow-up was 968 days in the febuxostat group and 942 days in the allopurinol group. The trial concluded that while treatment with febuxostat resulted in overall rates of major CV events that were similar to those associated with allopurinol treatment among patients with gout that have co-existing CV disease, it also reported that the CV death and deaths from any cause were more frequent in the febuxostat group than in the allopurinol group.
Based on the CARES trial, in 2019, the FDA placed the afore-mentioned black-box warning on febuxostat’s label. Was this warning premature? Dissecting the CARES trial further reveals the answer.
- Firstly, the CARES study compared febuxostat with allopurinol but included no control arm – thus, the febuxostat result is only interpretable relative to allopurinol in a patient population that inherently has a high risk of CV events without any interventions.
- Secondly, the CARES trial had a high drop-out rate with a majority of patients not completing the trial – subsequently, the data set is essentially incomplete.
- Thirdly, only a small fraction of the deaths occurred while patients were on the study drug. Specifically, about 90% of the reported deaths occurred after either febuxostat or allopurinol were stopped. Thus, it is difficult to attribute causality to a variable that was no longer present.
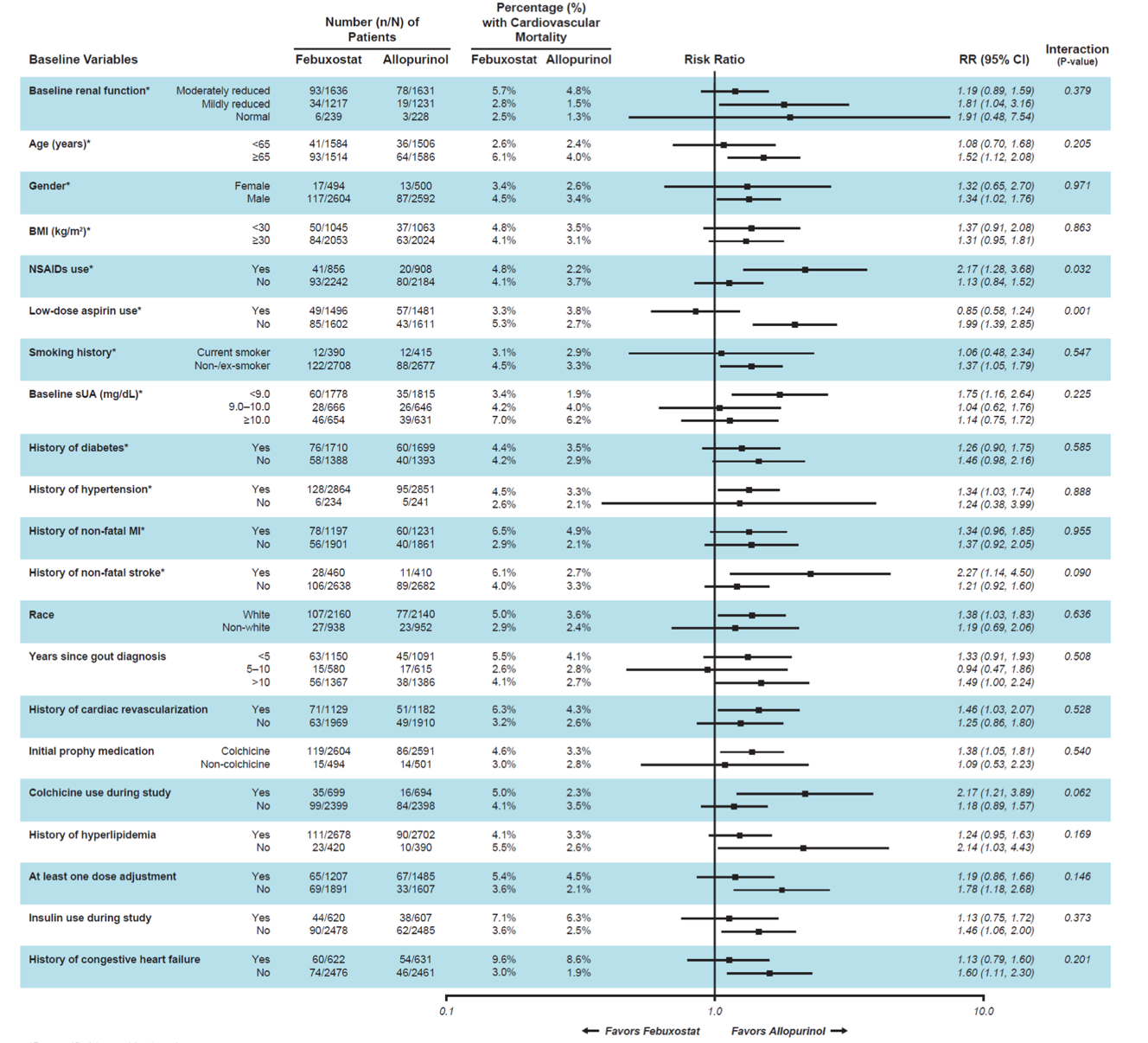
- Fourthly, the patients in the CARES trial had a higher risk of CV events (compared to other trials) yet not all patients were on cardioprotective aspirin. The trial also included patients on risk inducing NSAIDs. Although there was a twofold increased CV mortality rate for those patients that were randomly assigned to febuxostat without aspirin compared to those on allopurinol without aspirin, patients who were taking aspirin experienced no increase in rates of CV mortality while on febuxostat vs allopurinol. The opposite effect was seen with NSAIDs: patients randomly assigned to febuxostat who were also taking NSAIDs experienced a twofold increase in CV mortality compared with patients on allopurinol taking NSAIDs. However, there was no difference in CV mortality amongst either treatment arm in those not taking NSAIDs.
Figure S2. Risk Ratios for CV Mortality By Subgroups
A retrospective study by Zhang et al published in Circulation in 2018 looked at US Medicare claims data of 24,936 febuxostat initiators compared with 74,808 allopurinol initiators (roughly 100-fold the number of CARES cohort). The study showed that there was no difference between both groups in the incidence myocardial infarction and stroke (primary outcomes) or the secondary outcome of all-cause mortality.
A meta-analysis of 10 prospective trials by Cuenca et al published in the International Journal of Rheumatology in 2019 showed an increased rate of CV-associated rates of events but only when CARES study data was included.
In March 2019, the FREED study (a multicenter, prospective, randomized, open-label blinded endpoint) published in the European Heart Journal by Kojima et al included 1,070 elderly patients with hyperuricemia in an intention-to-treat population from 141 hospitals in Japan. FREED showed that febuxostat did not increase CVD, CV mortality, or all-cause mortality in this group of elderly patients at high risk of CVD compared to the low-dose allopurinol or no treatment arms.
The highly anticipated, late-breaking abstract (L#08), the FAST trial, by Mackenzie (& MacDonald) et al was presented at the 2020 American College of Rheumatology annual premier conference and published in The Lancet on November 9, 2020. It is a multicenter, prospective randomized, open-label, non-inferiority trial that shows that febuxostat is non-inferior to allopurinol with regard to the occurrence of major CV events over 4 years in 6,128 gout patients. Importantly, the study had a low rate of drop-out (~6%) compared to the high drop-out rate in CARES (~57%). Thus, the FAST trial results are essentially the antithesis of the results from CARES trial, and the FAST trial seems to put the controversy to rest in terms of the CV safety profile of febuxostat in patients with preexisting cardiovascular disease.
References:
CONFIRMS: https://pubmed.ncbi.nlm.nih.gov/20370912/
CARES: https://www.nejm.org/doi/full/10.1056/NEJMoa1710895
FREED: https://academic.oup.com/eurheartj/article/40/22/1778/5371086
FAST Study: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)32234-0/fulltext?






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.