

New insights in RA-ILD therapeutics Save


RA associated ILD (RA-ILD) is the most common extra-articular manifestation in RA. Its prevalence varies considerably, ranging from 5% to 30%, and is often underestimated since patients only become symptomatic or display abnormalities on chest X-Ray at a late stage of disease, leading to subsequent delay in diagnosis. In this context, several groups advocate for an earlier and more precise detection, using high resolution chest computed tomography (HRCT), which is the most sensitive for pre-clinical RA-ILD diagnosis. There has been a lot of fascinating presentations on RA-ILD so far at EULAR2021.
But why would we want to diagnose early a manifestation that we cannot treat?
While the effect of several cs and BioDMARDs on RA-ILD progression is still unclear, this year at #EULAR2021, two abstracts have examined the efficacy and safety of treatments in RA-ILD: the INBUILD trial #OP0124 presented by C. Kelly from Newcastle (Nintedanib) and the Treasure Registry looking at Tofacitinib (JAK 1/3 inhibitor) presented by U. Kalyoncu #OP0125.
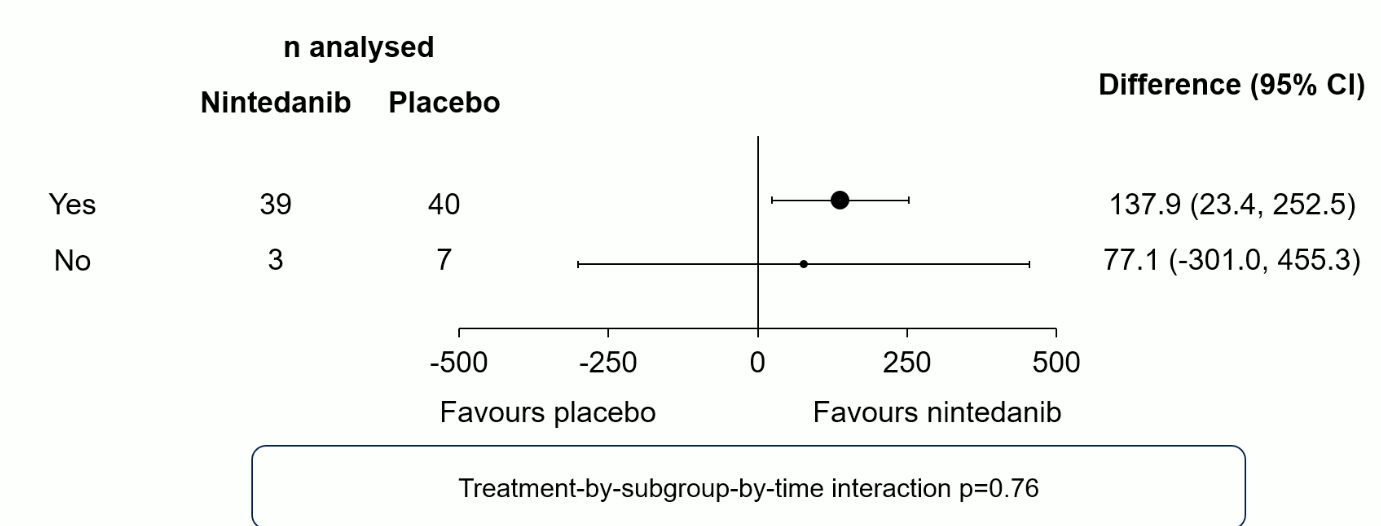
The population of 89 RA-ILD patients (>10% extent on HRCT, forced vital capacity (FVC) ≥45% predicted, diffusing capacity of the lungs for carbon monoxide ≥30%–<80% predicted) of the INBUILD trial (42 Nintedanib, 47 placebo) was typical: predominantly male (60.7%) current or former smokers (64.0%) were and 86.5% had a usual interstitial pneumonia (UIP)-like pattern on HRCT. The primary Endpoint, rate of decline in forced vital capacity (FVC) (mL/year) over 52 weeks was reduced significantly and in a clinically relevant manner (116.7 mL/year [95% CI 7.4, 226.1]; nominal p=0.037) in the Nintedanib group. Tolerance was satisfactory although retention rate was numerically reduced (19% vs. 12.8%) in the treatment group due to diarrhea mainly (54.8% vs. 25.5% PBO group).
Figure 1. Rate of decline in FVC (ml/years) over 52 weeks, in subgroups of patients with RA-ILD by use of DMARDs and/or GCs at baseline.
.
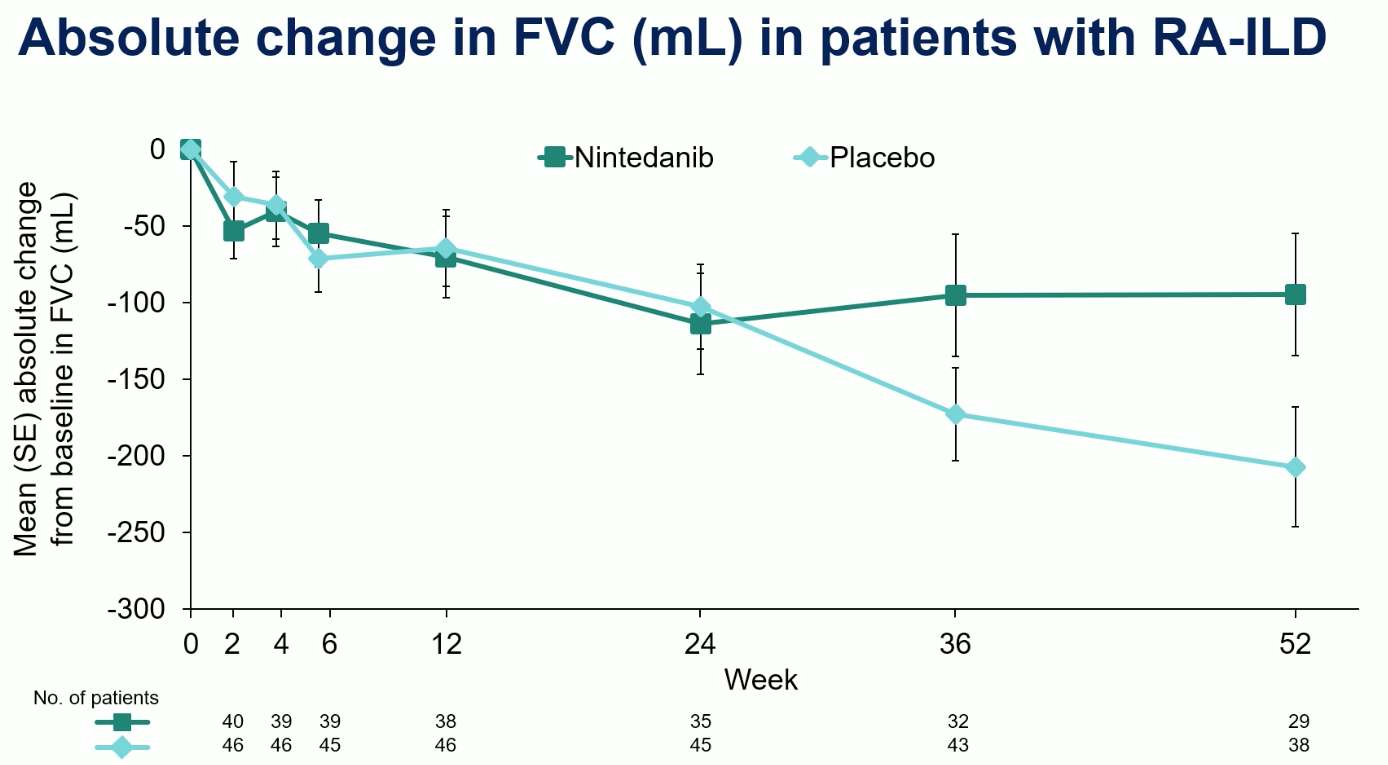
Figure 2. Absolute change in FVC over 52 weeks in both groups.
47 RA patients with RA-ILD and 387 RA non ILD patients from the TReasure registry were included for analysis. Since this is an observational study, conclusions regarding efficacy cannot be drawn however there was no degradation of the vital parameters mean FEV1% (82.1 vs. 82.8 pre and post-treatment, respectively, p=0.079), mean FVC% (79.8 vs. 82.8 pre and post-treatment, respectively, p=0.014). Retention rates were similar in both groups (p=0.21, log-rank). On the other hand, infection rate was numerically higher in the RA-ILD group leading to more superior rate of drug discontinuation (6.3 per 100 patient-years and 2.4 per 100 patient-years).
These abstracts although on limited numbers and potentially excluding the most severe patients (azathioprine, cyclosporine, mycophenolate mofetil, tacrolimus, rituximab, cyclophosphamide, or oral glucocorticoids >20 mg/day for #OP0124) provide new therapeutic insights into a yet poorly understood and difficult to treat RA manifestation. This represents hope for the future and should pave the way for larger RCTs in this heterogeneous and severe disease.






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.