

Review: Monoclonal Gammopathy of Undetermined Significance Save

NEJM has reviewed the common hematologic/immunologic finding of "monoclonal gammopathy of undetermined significance" (MGUS) - a common premalignant plasma-cell proliferative disorder found in approximately 5% of those over age of 50 years.
While MGUS may be a precursor to plasma-cell cancers, including multiple myeloma, solitary plasmacytoma, and Waldenström’s macroglobulinemia, it has also been linked to other serious nonmalignant disorders, collectively referred to as monoclonal gammopathy of clinical significance (MGCS).
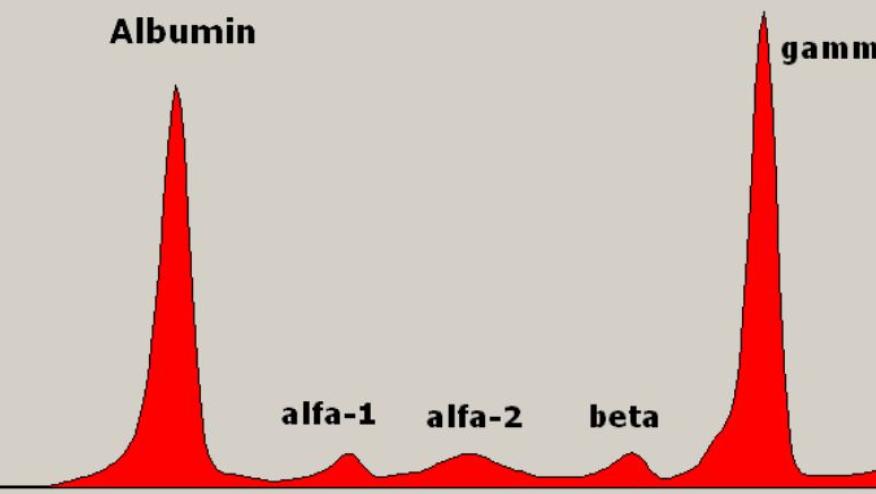
MGUS is characterized by a limited monoclonal proliferation of plasma cells secreting abnormal levels of immunoglobulins found as monoclonal (M) proteins on protein electrophoresis testing.
Most with MGUS or MGCS are asymptomatic (assuming no malignant transformation) but M proteins may cause serious harm with organ deposition.
Takeaways from this extensive overview:
- First recognized in the 1950s by Jan Waldenström ("essential hypergammaglobulinemia or benign monoclonal gammopathy"
- 1978, the term MGUS labeled Robert Kyle, noting this was not entirely benign and there may be a risk of malignant transformation
- MGUS can progress to cancer (multiple myeloma, Waldenström’s macroglobulinemia, solitary plasmacytoma) at a rate of 1% per year
- Bone marrow biopsy is not recommended for persons thought to have low-risk MGUS
- 2 main biologic types of MGUS: hyperdiploid MGUS and MGUS with IGH translocations (based on primary cytogenetic abnormalities — trisomies and translocations within the immunoglobulin heavy locus (IGH)
- Diagnosis is often incidental when M proteins are found as part of a broad workup in patients with fatigue, an elevated erythrocyte sedimentation rate, anemia, bone pain, osteoporosis, or infections.
- MGUS may also be diagnosed when multiple myeloma is considered in patients with osteolytic lesions, bone fractures, hypercalcemia, proteinuria, renal insufficiency, lymphadenopathy, or hepatosplenomegaly.
- MGUS is the premalignant precursor of myeloma, Waldenström’s macroglobulinemia, and solitary plasmacytoma
- MGCS may be associated wwith nephrotic syndrome, peripheral neuropathy, cardiomyopathy, amyloidosis, cryoglobulinemia, scleromyxedema, necrobiotic xanthogranuloma, and Schnitzler’s syndrome
- Treatment isn't necessary in MGUS; but may be dictated by a future neoplasia. Treatment of MGCS is based on the associated disorder.
- Evauation of MGUS should include a complete blood count and serum calcium and creatinine levels; and only do CT bone survey and bone marrow biopsy in those at higher risk
Continue Reading
ADD THE FIRST COMMENT
Disclosures
Disclosures
The author has no conflicts of interest to disclose related to this subject






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.