

Frailty in PMR: Why do I need to care? Save


First of all, what is frailty?
Frailty is a syndrome characterized by a decline in physiologic reserve, leading to an increased vulnerability to stressors and poor outcomes, including disability, falls, hospitalization, and mortality. Although initially described as a geriatric syndrome in community dwelling elderly, high prevalence of frailty has been reported in people living with different chronic conditions.
It is important to clarify that frailty is not a synonym of age (chronological age). Chronological age and biological age are not the same, and growing evidence points to the latter as a more appropriate assessment of adverse health outcomes of aging and increased risk of multiple geriatric syndromes including frailty. Frailty, similar to several other geriatric syndromes, has been independently associated to chronic levels of inflammaging (i.e., elevated levels of C-reactive protein, tumor necrosis factor-alpha receptor, interleukin-6) in community dwelling elderly. It is therefore not surprising that higher prevalence of frailty has been reported in different rheumatologic conditions and that there is a growing interest with regards to the impact of frailty in patients living with rheumatic diseases.
Why is frailty relevant in PMR?
Although there are only a few studies studying the impact of frailty in PMR, frailty is a relevant issue in this population due to several important factors:
- PMR primarily affects older adults
- Patients with PMR experience significant limitation in mobility and functional impairment due to ongoing pain and symptoms
- PMR is a chronic inflammatory condition
- Use of glucocorticoids, even for prolonged periods, is common in the treatment of patients with PMR and is associated with an increased risk of toxicity and morbidity
A single center study of 41 patients with PMR within the first year of diagnosis, found a prevalence of frailty and pre-frailty of 17% and 59%, respectively. Frail patients had worse physical function, and worse reported pain.1 Although there were no differences in inflammatory markers at time of assessment, frail patients with PMR had higher inflammatory markers at time of diagnosis, when compared to non-frail. There were no differences in disease activity as measured by the PMR-Activity Score.
In a recent study from Ireland that included 51 patients with PMR, 7.8% and 27.5% of patients were classified as frail and non-frail.2 Frailty patients were all female, and had a higher body mass index compared to pre-frail and non-frail patients. Frail patients had worse patient-reported outcomes for mood, pain, fatigue and overall quality of life.
Although more work is needed, these studies show that frailty in PMR is associated with worse pain, physical function, and fatigue - all clinically relevant symptoms in people living with PMR.
How to measure frailty?
Currently, there is no consensus on measures. Most of the definitions do involve specific testing that is more suitable and feasible to the research setting. However, simpler measures, and two examples include:
- Gill Frailty measure: Gait speed and ability to stand from the chair
- FRAIL scale: Self-administered 5-item questionnaire3
The FRAIL scale has shown a good correlation with more standard research tool for the assessment of PMR and represents a simple and quick tool that can be easily implemented in medical care.4
Although implementation might be challenging, awareness of the concept and discussion of frailty with PCP or geriatricians is important in this age group.
What to consider in the care of frail older adults with PMR?
- Consideration of physical therapy and occupational therapy: Physical activity interventions are beneficial in frail patients, and although these should be considered in all patients with PMR, frail individuals should certainly be prioritized. Referral to physical and occupational therapy should be discussed and recommended, and this can help with improving mobility, management of chronic pain, and gait/stability interventions to prevent falls.
- Medications and polypharmacy: a common problem in older adults, especially frail older adults. Medication-related adverse events, including glucocorticoid-related, should be closely monitored in this group.
- Ask about falls: frail individuals are at higher risk of falls and complications. Simply asking “Do you feel unsteady when standing or walking?” and “Have you fallen in the last year?” are good screening questions to assess for fall risk.
- Assessing for depression: consider screening with the PHQ-2, asking how often have they been “having little interest or pleasure in doing things” or “feeling down, depressed, or hopeless” in the past 2 weeks?
- Communication with primary care and/or geriatrician: coordination of care is crucial for all patients, particularly frail older adults. If there is a concern for frailty and risks with treatment or disease, referral to geriatricians should be considered.
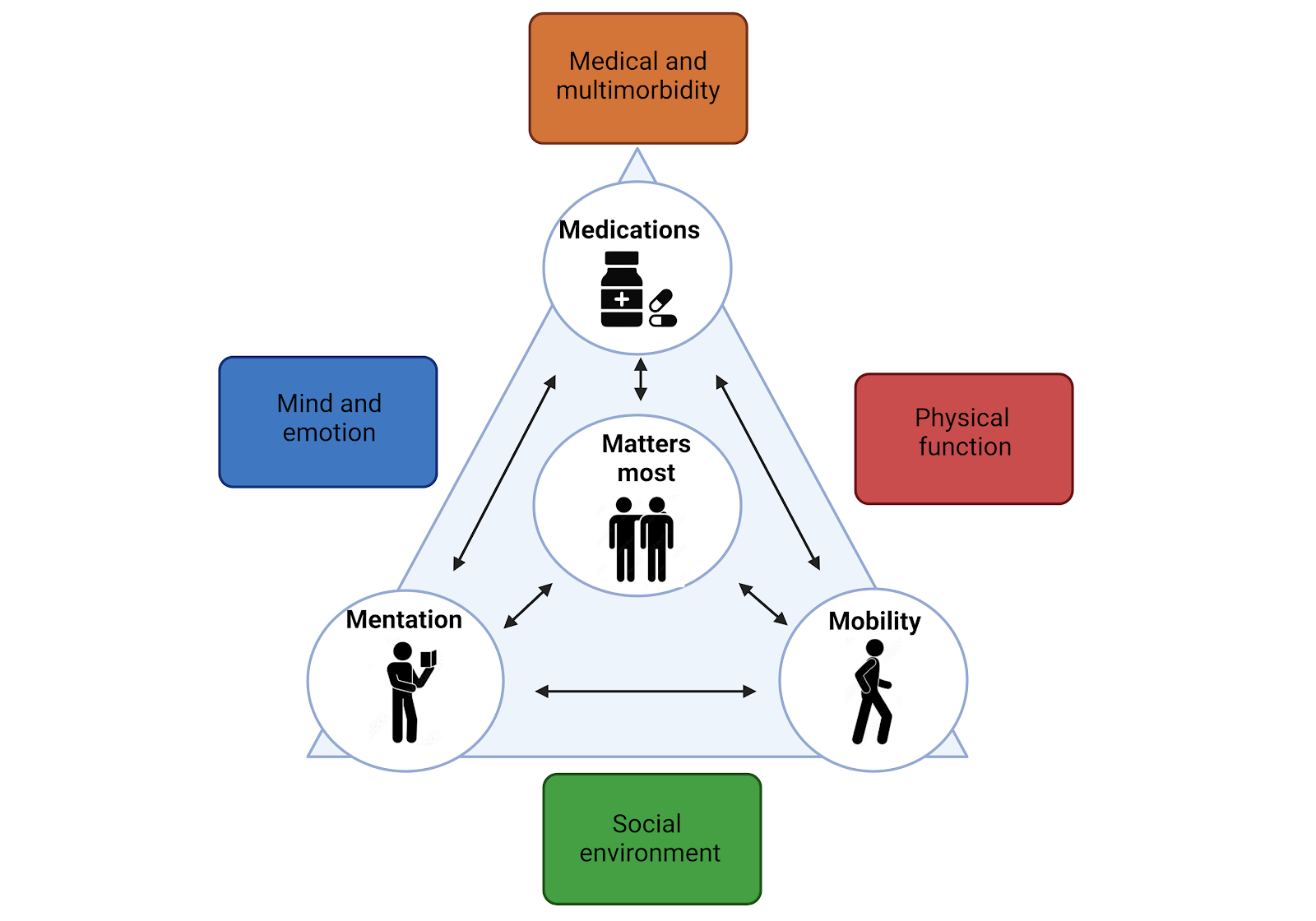
Several of these concepts are englobed within the 5M framework of geriatrics (see figure), though I have not covered them all above. The 5Ms represent a useful and holistic approach to the care of older adults that should be considered in the care of all older adults living with rheumatic diseases.
Adapted from Goyal P. JACC Adv. 2022. Figure created with Biorender.
References.
1. Sattui SE, Jannat-Khah D, Lally L, Lieber SB, Mandl LA, Spiera RF. Prevalence of frailty in patients with polymyalgia rheumatica and association with health-related quality of life, cognition and sarcopenia. Rheumatology (Oxford). 2022 Nov 2;61(11):4455-4464. doi: 10.1093/rheumatology/keac050. PMID: 35136992; PMCID: PMC9629413.
2. Harkins P, Cowley S, Kane D, Conway R. Frailty and Its Impact on Patient Reported Outcomes in Polymyalgia Rheumatica [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/frailty-and-its-impact-on-patient-rep…. Accessed October 10, 2023.
3. Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. 2012 Jul;16(7):601-8. doi: 10.1007/s12603-012-0084-2. PMID: 22836700; PMCID: PMC4515112.
4. Sattui S, Jannat-Khah D, Lally L, Lieber S, Mandl L, Spiera R. Assessment of a Patient Self-Report Frailty Tool in Patients with Polymyalgia Rheumatica [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/assessment-of-a-patient-self-report-f…. Accessed October 11, 2023.
ADD THE FIRST COMMENT






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.