Prescribing Lessons (4.17.2026)
Dr. Jack Cush reviews the news and journal articles from this past week on RheumNow.com.
Read Article


Dr. Jack Cush reviews the news and journal articles from this past week on RheumNow.com.
Read Article

An NEJM study has shown that glucocorticoids provide no added benefit when added to standard primary treatment in Kawasaki disease patients.
Read Article
Biogen has announced positive results of their Phase 2 study, evaluating litifilimab in patients with active cutaneous lupus erythematosus (CLE), presented at the recent American Academy of Dermatology (AAD) Annual Meeting.
Litifilimab is an investigational monoclonal antibody that
Read Article
JAMA has published a current Clinical Guidelines Synopsis on the Management of Crohn Disease (CD) in Adults.
Read Article
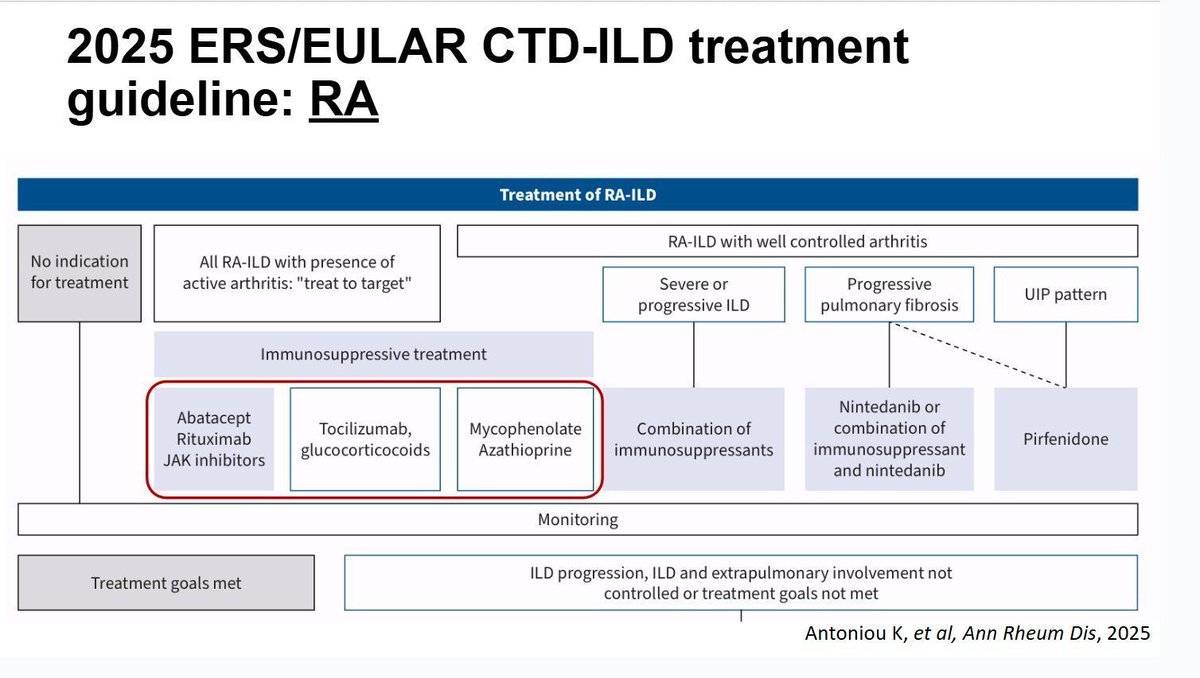
RA-ILD represents the most severe extra-articular manifestation of rheumatoid arthritis, affecting an estimated 1% of the adult population in the US and Northern Europe. Prevalence estimates vary widely (up to 58%), reflecting different diagnostic criteria, imaging modalities, and study
Read Article
Dr. Jack Cush reviews the journal reports and news from RheumNow.com. This week we discuss moral distress, FM in PsA, Lyme Vax is back & hidden but tangible benefits of the MDHAQ.
Read Article
EULAR has updated its recommendations for the management of Behçet’s syndrome, the last being published in 2018. The current update carries no recommendations from the previous version: seven recommendations have content modifications, four have minor wording amends, and one is entirely new
Read Article
Prednisone use in Alberta primary care 546 #RA pts - 40% of PCP RA Rx w/ 1 or more prednisone Rx. 41% Rx w/ both Pred + DMARD, w/ 44% on Pred median 124 day before DMARD. 66% continued Pred >1 yr after DMARD initiation. https://t.co/wrxQRP2TWN https://t.co/XxWpjafBsk
Links:
Dr. John Cush @RheumNow( View Tweet )
The European Alliance of Associations for Rheumatology (EULAR) has updated their rheumatoid arthritis (RA) management recommendations, notably with fewer recommendations (total of 9, down from 11 in 2022 version), by merging and removing previous recommendations.
Read Article



I recently attended a fascinating lecture by Dr. Anisha Dua on progress in the diagnosis and treatment of large-vessel vasculitis, with a focus on giant cell arteritis (GCA) and Takayasu's arteritis. She opened with what felt like the most honest “state of the union” slide you can show a room
Read Article
Dry eye rates upwards of 20% were seen across nine common autoimmune diseases other than Sjögren's, most often in rheumatoid arthritis (39.3%) with Crohn's disease bringing up the rear (23.0%), according to Chi-Chin Sun, MD, PhD, of Chang Gung Memorial Hospital in Keelung, Taiwan, and colleagues
Read Article
Dr. Jack Cush reviews the hot item takeaways from last week's RheumNow.Live 2026.
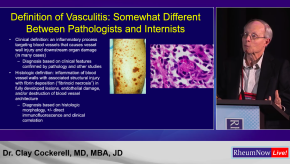
Sunday’s vasculitis session at RNL26 was a fantastic update on inflamed blood vessels, large and small, by two experts in the field: rheumatologist Dr. Mike Putman and dermatopathologist Dr. Clay Cockerell.
Read Article
Dr. Jack Cush reviews the news, journal articles and regulatory news from this past week on RheumNow.com
Read Article
How would you manage a patient with Overlap (anti-synthetase) syndrome, ILD, polyarthritis and myositis?


By downloading this material, I acknowledge that it may be used only for personal use and personal education and that I will accredit RheumNow.com as the source and owner of this material. Commercial use or mass reproduction of this material without permission from RheumNow (info@rheumnow.com) is prohibited.