

Blogs

Best of 2023: PMR: glad or bad tidings?
Please don’t tell your patient that PMR “typically” lasts two years. According to real-world data from the UK, one in four patients with PMR is prescribed steroids by their primary care physician for over four years. But nobody tells them this at the start, and that causes big problems later on.
Choice Overload (and the Way Out)
I recently overheard a very good practicing rheumatologist complain, “why do I need yet another drug for psoriatic arthritis? I have more treatment choices than I have actual PsA patients who need a new or better drug”.
Advancing PMR
Even though polymyalgia rheumatica is not perceived by many physicians as a severe diagnosis, its diagnosis and management actually propose significant challenges. I'd like to talk about those challenges, and what directions our path forward can include to advance our understanding and improve the treatment of patients who have PMR.
JAKi for PMR: Safe, or a Concern for Older Adults?
JAK inhibitors obviously have dominated a lot of the discussion in our therapeutic landscape over the last couple of years. What about their use in polymyalgia rheumatica? Let's consider.
When PMR Strikes Young, It Hits Hard
Narratives around polymyalgia rheumatica (PMR) often centre around “older people” or even “elderly”. And, indeed, the peak of the age distribution is in the mid-70s – not that everyone that age considers themselves old. Treating “young PMR” can be a very different proposition to treating someone in their seventies or eighties. It’s worth taking time to think this through.
Impact of glucocorticoids: more than just toxicity
As the sole effective treatment for polymyalgia rheumatica since their development in the 1950’s until recently, the impact of glucocorticoids and PMR outcomes are undeniably intertwined. So much so that when the OMERACT PMR working group first set out to develop a PMR core outcome set, they quickly realised that many of the outcomes important to patients were related to their glucocorticoid use.

Universal Imaging for GCA in PMR? Not So Fast
For decades we've been screening GCA with a patient history and exam. Doing so with imaging would be a sharp departure from the current standard of care. And you may be asking yourself, well, yeah, but what could it hurt? Don't you want to catch GCA early? Let me tell you the problems with this.
Unpopular opinion: spinach can be bad for you
PMR might be one of the most rewarding diagnoses to make in real practice: the patient comes to you in severe debilitating pain, and you prescribe steroids, giving them their lives back! As much as this impressive response makes your intervention appear almost magical, there is the often-forgotten story about the implications of such a diagnosis and treatment on patients' daily lives.
What Causes PMR?
What causes polymyalgia rheumatica? It could be said that PMR occurs when trajectories of aging take a wrong turn, but it’s still not clear exactly what it is that causes this to happen. The ideas that follow will doubtless seem, to immunologists, vague and oversimplified; but even a partial picture might still offer a possible framework for clinicians and patients for thinking about treatment and care.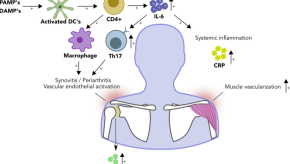
What Goes Wrong with the Immune System in PMR?
Polymyalgia rheumatica (PMR) is a common inflammatory rheumatic disease. The exact trigger for PMR onset remains unknown. However, immunology studies and clinical trials with biological DMARDs now shed light on the immune pathways involved in PMR.

