

2025 Update: EULAR Recommendations on Rheumatoid Arthritis Management Save

The European Alliance of Associations for Rheumatology (EULAR) has updated their rheumatoid arthritis (RA) management recommendations, notably with fewer recommendations (total of 9, down from 11 in 2022 version), by merging and removing previous recommendations.
An International Task Force was formed to review new evidence and update the 2022 guidance. This update has 5 overarching principles and 9 recommendations concerning use of conventional synthetic DMARDs, biological (b)DMARDs (including biosimilars) and targeted synthetic [ts]DMARDs. Guidance on treatment strategies (treat-to-target), and tapering with clinical remission is provided. Safety aspects, costs and sequencing of b/tsDMARDs were considered.
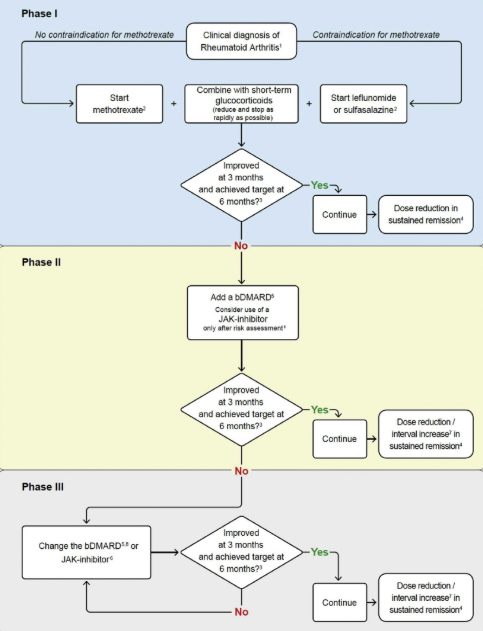
- For RA, MTX ideally in combination with short-term GCs is recommended; but if there is an insufficient response after 3 to 6 months, a bDMARD should be added. This could include a JAK inhibitor after careful consideration of risks (MACEs, malignancies and/or thrombo-embolic events).
- If the first bDMARD (or JAKi) fails, any other bDMARD (from another or the same class) or JAKi (considering risks) is recommended.
- With sustained remission, DMARDs may be tapered, but caution is required as stopping often leads to a flare.
The authors reiterated that remission is the main target in all patients, especially in thosewith early disease. However, low disease activity can be an alternative goal, especially in patients with long-standing disease who already have failed 1 or more previous DMARD therapies. Any state other than low disease activity should be regarded as unacceptable,
Overartching Principles (remained the same)
- Treatment of patients with RA is aimed at the best care and must be based on shared decision making between the patient and the rheumatologist.
- Treatment decisions are based on disease activity, safety issues and other patient factors, such as comorbidities and progression of structural damage.
- Rheumatologists are the specialists who should primarily care for patients with RA.
- Patients require access to multiple drugs with different modes of action to address the heterogeneity of RA; they may require multiple successive therapies throughout life.
- RA incurs high individual, medical, and societal costs, all of which should be considered in its management by the treating rheumatologist.
Guidelines
- Therapy with DMARDs should be started as soon as the diagnosis of RA is made.
- Treatment should be aimed at reaching a target of sustained remission or low disease activity in every patient.
- Disease activity monitoring+ should be frequent in active disease (every 1-3 mo); if there is no improvement by at most 3 mo after the start of treatment or the target has not been reached by 6 mo, therapy should be adjusted; when the target is sustained, monitoring can be less frequent
- MTX should be part of the first treatment strategy; in patients with a contraindication to MTX (or early intolerance), leflunomide or sulfasalazine should be considered.
- Short-term glucocorticoids should be considered when initiating or changing csDMARDs, in different dose regimens and routes of administration, but should be tapered and discontinued as rapidly as clinically feasible
- If the treatment target is not achieved with the csDMARD strategy, a bDMARD should be added; JAK inhibitors may be considered, but pertinent risk factors* must be taken into account.
- bDMARDs/tsDMARDs should be combined with a csDMARD; in patients who cannot use csDMARDs as comedication, IL-6 pathway inhibitors and JAK inhibitors may have some advantages compared with other bDMARDs.
- If a bDMARD or tsDMARD has failed, treatment with another bDMARD or a tsDMARD+ should be considered; if 1 TNF or IL-6 receptor inhibitor therapy has failed, patients may receive an agent with another mode of action or a second TNF-/IL-6R-inhibitor
- After glucocorticoids have been discontinued and a patient is in sustained remission, continuation of DMARDs (bDMARDs/tsDMARDs and/or csDMARDs) is recommended, but dose reduction may be considered.
ADD THE FIRST COMMENT
Disclosures
Disclosures
The author has no conflicts of interest to disclose related to this subject






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.