

Best of 2025: 2025 BSR Guideline for Treatment of Axial Spondyloarthritis Save

Editor's note: This article was originally published April 22, 2025, and is being shared again as part of RheumNow's 'Best of 2025' series as we close out the year. Enjoy!
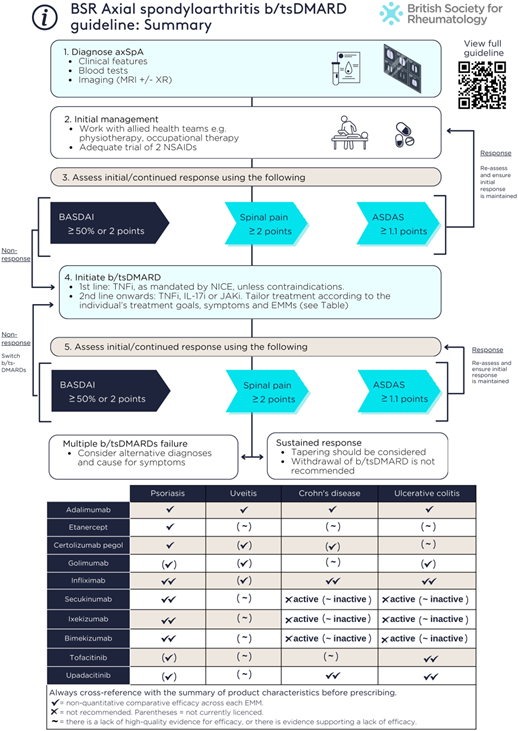
The British Society of Rheumatology has published its 2025 Guidelines for the Treatment of Axial Spondyloarthritis (axSpA); addressing axial and extra-musculoskeletal manifestations including acute anterior uveitis, psoriasis and IBD. They address the effectiveness and safety of targeted therapies; switching, combining, tapering or withdrawing targeted therapies; and treating to target. The guideline applies only to adults with axSpA. Biologic and targeted synthetic DMARDs (b/tsDMARDs) are referred to as “targeted therapies”.
The guideline includes 3 overarching principles and 15 guideline recommendations.
Overarching principles
- The primary goal of treatment is to enable patients, optimize quality of life, prevent structural damage, and preserve physical function, work productivity and social participation
- Shared management decisions should be developed between patient and provider
- Management should involve a multidisciplinary team, a holistic approach and use both pharmacological and non-pharmacological interventions
Recommendations
- TNF, IL-17 or JAK inhibitors are recommended for people with active axSpA who have not responded adequately to non-pharmacological and conventional pharmacological management
- Active disease should be determined by the treating clinician in the context of verified diagnosis and inflammatory disease activity
- Response to targeted therapies should be assessed using validated indices (e.g. ASDAS, BASDAI, spinal pain) 3–4 months after initiation, and every 6–12 months if treatment is continued.
- The absence of response to targeted therapies should prompt reassessment of the diagnosis and the extent of inflammatory disease activity
- An alternative targeted therapy is recommended for individuals with active disease who cannot tolerate, do not respond to, or lose response to the initial targeted therapy
- In the presence of moderate-to-severe or recurrent uveitis, a monoclonal TNFi is preferred over therapies with other mechanisms of action
- A history of inactive uveitis is not an absolute contraindication to therapies with other mechanisms of action
- If new uveitis develops in the context of well-controlled axSpA, decisions to change treatment should be made with an ophthalmologist where possible, taking into account the severity and/or frequency of uveitis flares and response to topical steroid
- IL-17 and monoclonal TNFi are preferred in the presence of extensive psoriasis (e.g. >10% body surface area) or severe localized psoriasis at sites associated with high functional impairment or impact (e.g. face, scalp, palms, soles, flexures, genital or nails), ideally in conjunction with a dermatologist
- Individuals with unexplained lower gastrointestinal symptoms should be assessed by a gastroenterologist, ideally before commencing targeted therapies
- In the presence of active IBD, monoclonal TNFi or JAKi are preferred; IL-17 inhibitors should not be commenced
- A history of inactive IBD is not an absolute contraindication to IL-17 inhibitors or etanercept
- Treatment should aim to achieve predefined targets agreed upon with the individual living with axSpA, using individualized therapy adjustments that consider comorbidities and inflammatory disease activity
- Tapering of targeted therapies should be considered for individuals who have achieved sustained remission
- Withdrawal of targeted therapies in the context of sustained remission is not recommended
The areas the guideline does not cover
- NSAIDs, glucocorticoids and conventional synthetic DMARDs.
- Treatment of enthesitis/spondylitis-related juvenile idiopathic arthritis.
- Axial disease in psoriatic arthritis.
- Safety of targeted therapies or their use in pregnancy
- Health economic considerations.
ADD THE FIRST COMMENT
Disclosures
Disclosures
The author has no conflicts of interest to disclose related to this subject






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.