

Methylprednisolone plus Methotrexate in Giant Cell Arteritis Save


What is the optimal glucocorticoids (GC) regimen in giant cell arteritis (GCA)? Does methotrexate (MTX) work in GCA?
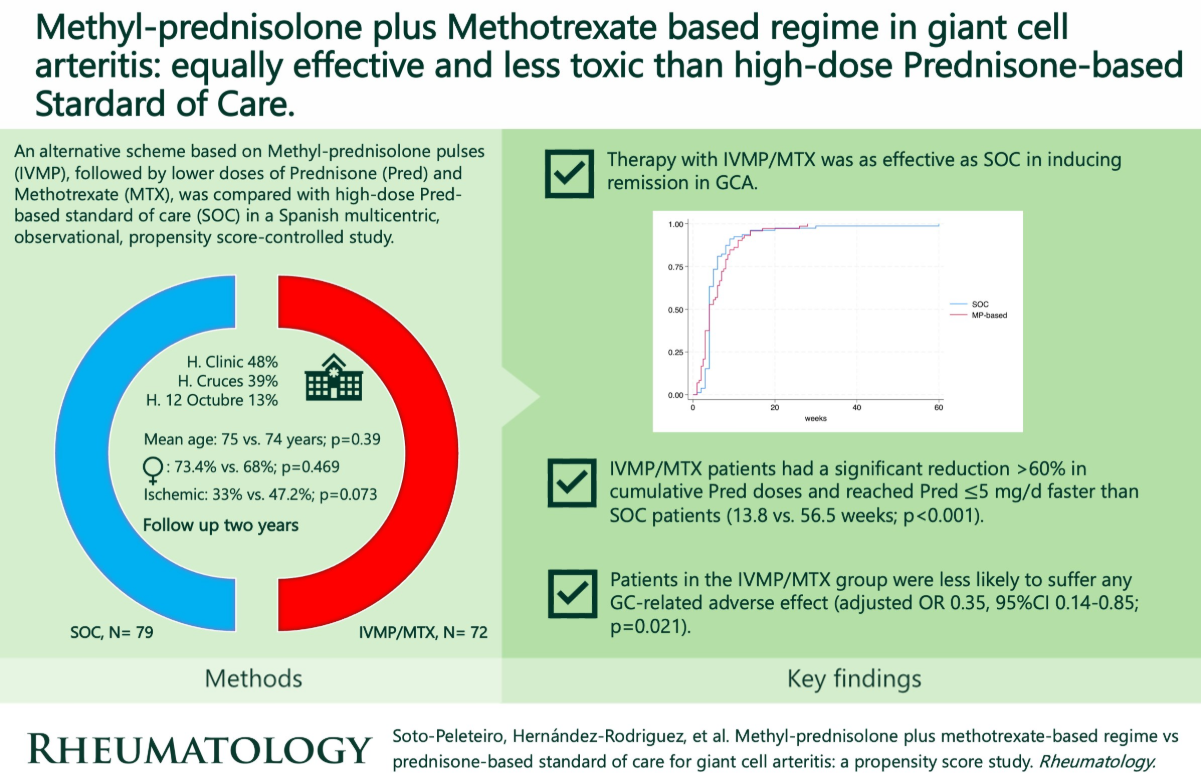
A multicenter trial from Spain shows equivalent outcomes when GCA patients were treated with a combination of intravenous methyl-prednisolone (IVMP) pulse plus MTX compared to GC alone (standard of care/SOC). They concluded that combination IVMP/MTX with lower-dose prednisone is as effective as the SOC, but had less overall GC exposure.
A total of 151 GCA patients were treated with SOC-prednisone (40–60 mg/d) or with IVMP (125–500 mg/d x3) followed by lower-dose prednisone (≤30 mg/d) and MTX (IVMP/MTX). After a follow-up of 2 years and propensity score matching, the primary outcome was GCA remission.
Both groups were similar at baseline. Observed outcomes included:
- 100% patients in both groups achieved remission after a median time of 4 weeks
- Relapse rates were also similar.
- IVMP/MTX had significantly lower cumulative GC doses and reached prednisone ≤5 mg/d faster than SOC (13.8 vs 56.5 weeks; p< 0.001).
- IVMP/MTX group had fewer GC-related adverse effect (adjusted OR 0.35, 95%CI 0.14–0.85; p= 0.021).
Both regimens were effective, but IVMP/MTX significantly reduces GC exposure and GC-associated adverse effects.
ADD THE FIRST COMMENT
Disclosures
Disclosures
The author has no conflicts of interest to disclose related to this subject






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.