

Is Your Practice Up to Date? New Guidelines for SLE Nephritis Save

Randomized controlled trials (RCTs) drive guidelines; guidelines drive clinical practice. Because updated guidelines lag trials by many years and dissemination of guidelines takes additional time, rheumatologists often practice “behind the data.” The 2024 ACR Guidelines for the Management of SLE Nephritis reaffirmed many of our typical practice patterns, including hydroxychloroquine for all, renin/angiotensin blockade, and favoring mycophenolate mofetil over cyclophosphamide. They also presented an excellent opportunity to step back and ask, “Have I updated my practice to accommodate new data?”
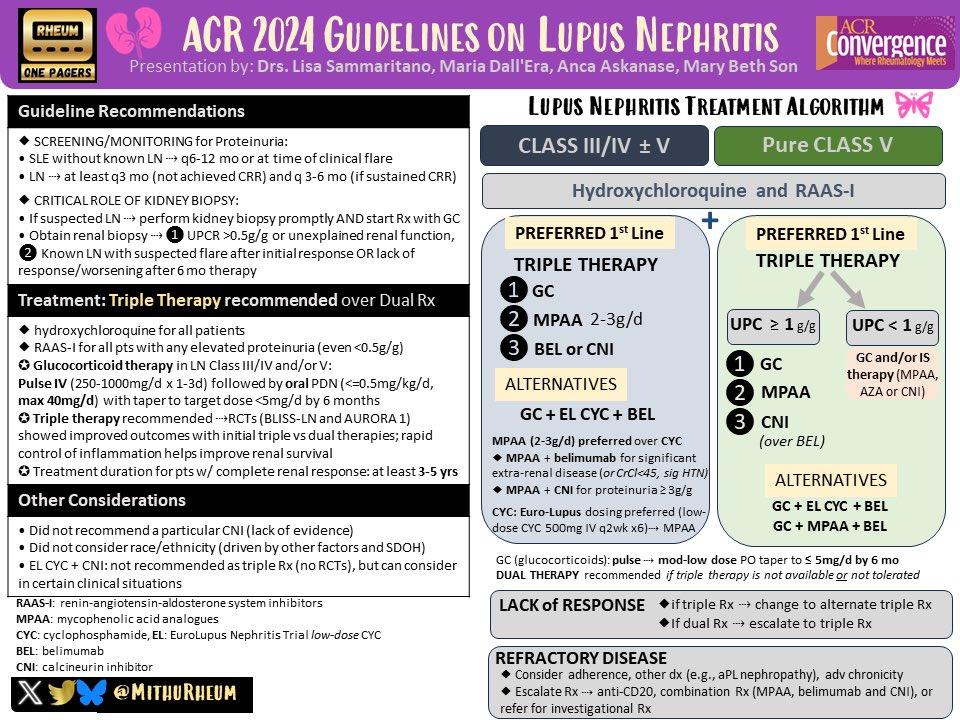
Figure 1: Updated ACR Guidelines for SLE-LN, courtesy of Mithu Maheswaranathan, MD
First and foremost, how much steroid should patients with SLE-LN receive? Many of us have long practiced within a “1mg/kg and taper” paradigm, which results in substantial steroid exposure and adverse events. Patients wind up on steroids far longer than we expect (Abstract 0168), receive DMARDs less frequently than they should (Abstract 0667), and experience glucocorticoid related side effects (Abstract 0179 and Abstract 364). Reducing steroid exposure – to whatever extent possible – is a laudable goal.
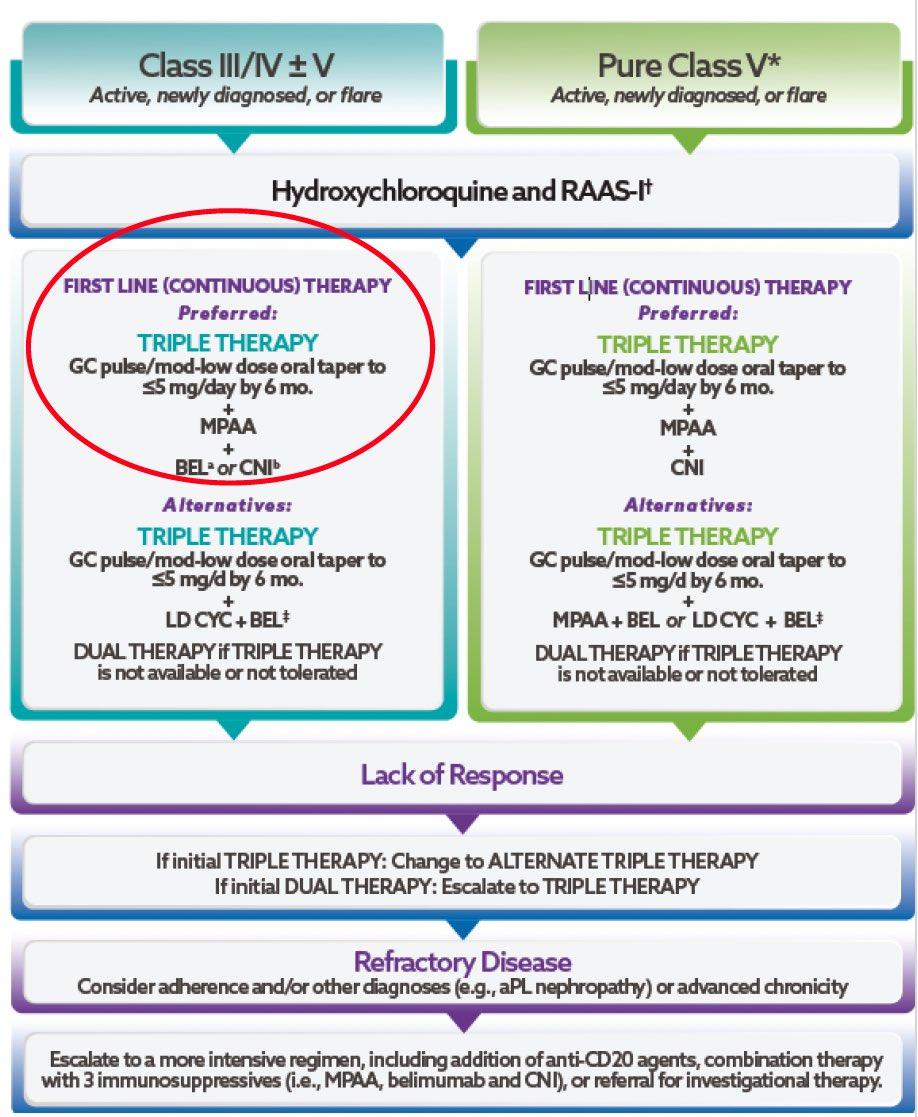
The new ACR guidelines have embraced a much faster taper than the prior version, recommending an initial dose of 0.5mg/kg per day and a taper to <=5mg by 6 months. This brings ACR guidelines into alignment with the 2019 and 2024 EULAR guidelines, which recommended 0.3-0.5mg/kg per day, tapered to <=5 by 3-6 months. It may also make rheumatologists uncomfortable, and for good reason! A recent evaluation of steroid tapers from randomized trials observed an association between lower dose regimens and a lower rate of remission. The flip side is that nothing comes free; higher initial-dose tapers were associated with higher rates of infection and death. Steroid risks and benefits are dose dependent; shifting your practice will necessarily get more or less of both.
If you are feeling uncomfortable with a reduced dose steroid taper, replacing some of that immunosuppression with “Triple Therapy” may help. The recently published BLISS-LN (belimumab in SLE-LN) and the AURORA (voclosporin in SLE-LN) trials established the value of adding one of these DMARDs to our prior standard of care (glucocorticoids + mycophenolate mofetil). The updated guidelines favor a calcineurin inhibitor for patients with pure Class V nephritis, which makes sense to me given the clear benefit to proteinuria from AURORA (caveat: also a benefit in BLISS-LN). They remain agnostic about which to choose for patients with Class III/IV +/- Class V, but I personally favor belimumab for patients whose EGFR has been meaningfully affected.
I always say “guidelines are meant to be broken,” so where would I deviate from these? First, I am uncomfortable with pulse dose steroids. The guidelines and the aforementioned analysis of RCT steroid tapers suggested “pulse upfront plus low dose taper” could be an optimal regimen, but for patients with milder disease I would be hesitant to provide one.
Second, I am an “MMF First” kind of guy, but cyclophosphamide needs to be in your toolkit (the guidelines acknowledge this). I typically favor cyclophosphamide for patients with extra-renal manifestations, such as myocarditis or central nervous system involvement, and typically titrate the dose to the acuity of the presentation (EUROLUPUS protocol for less sick; NIH or CYCLOPS for people with life threatening presentations).
Finally, remember that patient preference will always be paramount. The best drug is the one that your patients take; the healthiest patients are the ones who trust your judgment and come back to see you again. Finding the right balance may mean favoring calcineurin inhibitors over belimumab (people like pills better than injections) or foregoing either entirely if it increases the chances your patient will adhere to our “old” triple therapy of HCQ + prednisone + MMF.
One final plug: if you would like something to print for your office, I highly recommend this “One Pager” by Mithu Maheswaranathan!






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.