

Cryoglobulinemic Vasculitis Reviewed Save

Cacoub et al review the common entity cryoglobulinemic vasculitis (CryoVas) in the current issue of the American Journal of Medicine.
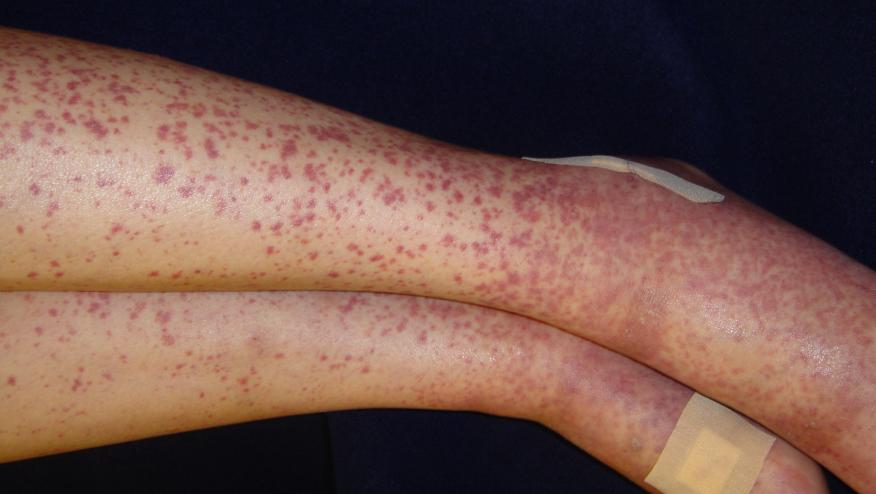
This small-vessel vasculitis involves the skin, joints, and potentially other organs, including the peripheral nervous system or the kidneys.
Cryoglobulins are classified as types I, II and III. Type I are single monoclonal immunoglobulins often related to an underlying B-cell lymphoproliferative disorder. Type II (mixed monoclonal and polyclonal), or type III (mixed polyclonal), are often referred to as mixed cryoglobulinemia. These may have polyclonal immunoglobulin (Ig)G with or without monoclonal IgM and rheumatoid factor activity. Hepatitis C virus (HCV) infection represents the main cause of mixed CryoVas.
The 10-year survival rates range from 63%, to 87%. In HCV-positive CryoVas, poor prognostic factors include the presence of severe liver fibrosis, and CNS, kidney, and cardiac involvement. Treatment with antivirals is associated with a good prognosis, whereas use of immunosuppressants (including corticosteroids) is associated with a poor outcome.
In HCV-negative patients, pulmonary and gastrointestinal involvement, renal insufficiency, and age > 65 years are independently associated with death. Increased risk of lymphoma also should be underlined.
Treatment of type I CryoVas is that of the hemopathy; specific treatment also includes plasma exchange, corticosteroids, rituximab, and ilomedine. In HCV-CryoVas with mild-to-moderate disease, an optimal antiviral treatment should be given. Rituximab may be considered in HCV-CryoVas for severe vasculitis should be given before initiation of antiviral therapy.
Continue Reading
ADD THE FIRST COMMENT
Disclosures
Disclosures
The author has no conflicts of interest to disclose related to this subject






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.