

ANA Rules Save
By downloading this material, I acknowledge that it may be used only for personal use and personal education and that I will accredit RheumNow.com as the source and owner of this material. Commercial use or mass reproduction of this material without permission from RheumNow (info@rheumnow.com) is prohibited.
Body
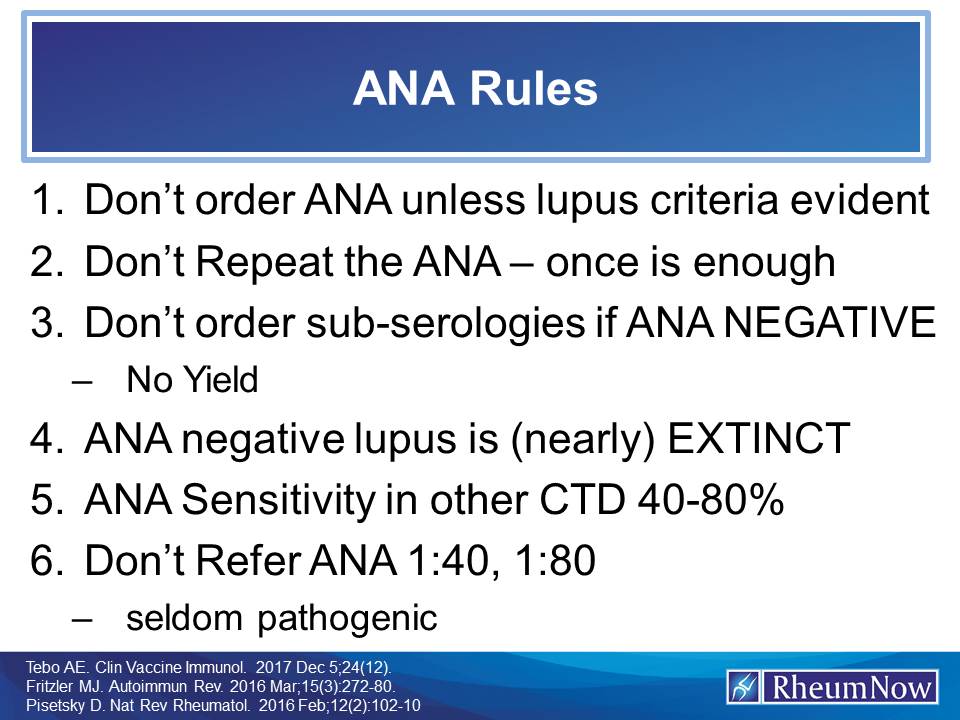
How to use ANA tests
Join The Discussion
Comments
I don’t agree with any of the rules.
1) doorder ana if no clinical lupus.ANA may be helpful for RA, sjogrrns, scleroderma, myositis
2)repeat ANA. It comes and goes
3)order subserologies. ENA, SSA,SSB. Very helpful may show lupus.
4) absolutely not. Look at new studies showing up to 24% Ana negativity in established lupus.
5) Ana neg RA, other ctd, even sle is seen.
6) do refer low pos Ana if PAIN is present. It is very helpful in outcome, response to dmard.
Thank you.
1. You cannot diagnose RA with an ANA. ANA are absent in half of PSS and PM/DM patients. 2. If ANA comes and goes - your doing it too often and finding useless information. 3. If you regularly diagnose and treat lupus with a negative ANA then your neglecting 50 years of ANA research. 4. Seems i have rigid rules for the use of ANA that you do not. Best wishes JJC
Dr Cush thank you for your reply it is very nice to interact with you I follow your weekly reviews religiously and appreciate them.
1) Ana may be neg in non lupus ctd but when positive it helps. So if no clinical lupus, still order Ana if ctd is suspected.
2)I don’t think Ana that comes and goes is useless. I’ve diagnosed ctd including lupus in currently Ana neg past Ana pos or vice versa pts. So if it is neg it may be pos in future or may have been pos in past. That changes my approach if cro is also elevated especially.
3)I dontctegularly diagnose or treat lupus with a neg Ana. I don’t believe in ruling out lupus if clinical signs are present Ana neg due to #2 above.4) I think rules can be bent or may prove less rigid my 18 years in Rheumatology has taught me this . Maybe another 18 years will teach me the opposite. I will live and learn, again very nice talking with you Ulker.
how old was the oldest patient that you have made a new dx of lupus? I get request for referrals for patients in their geriatric years with joint pain and +ANA.
Dr. Cush. I'm a PCP, not a Rheumatologist. I know you state not to repeat the ANA, but what about following a patient with significantly elevated ANA (say 1:320), and not quite meeting criteria for lupus. Should these patients at least be followed q12 months by a rheumatologist for subsequent progression to lupus or other CTD, which may be around 18% of cases (https://rheumnow.com/content/predicting-autoimmune-progression-ana-pati…)
Also, regarding sub-serologies, the Choosing Wisely program suggests that at least checking Jo1 and SSA in appropriate situations may still be valuable.
https://www.choosingwisely.org/clinician-lists/american-college-rheumat…
Thoughts?
Thanks for this question. At the core of my teaching slide is the notion that the ANA is a confirmatory test (based on having lupus like symptoms - beyond aches or pains); it is a horrible diagnostic test if used to screen for disease that might be lupus or autoimmune. An ANA of 1:320 is still a low positive that is meaningless if there arent SEVERAL lupus specific features in play. I dont and wouldnt repeat the test (to see where it goes) unless the patients symptoms and status evolves to more SLE features, and then... ordering an ANA is helpful and confirmatory. Ordering subserologies (Jo1 or SSA) if the ANA is negative is a mistake and unwise advise, as the diagnostic yield would be very very very low.
Bottom line - if the patient has pain (& you dont know why) and you find a +ANA (& your wondering if its lupus) -- it would be smart to refer to rheumatology to find out the cause of the pain (usually easier for rheum to explain the pain, than to try to fit the pain and low ANA into an unreasonable SLE diagnosis).






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.