

What Lies Beneath: Understanding Nailfold Capillaroscopy Save

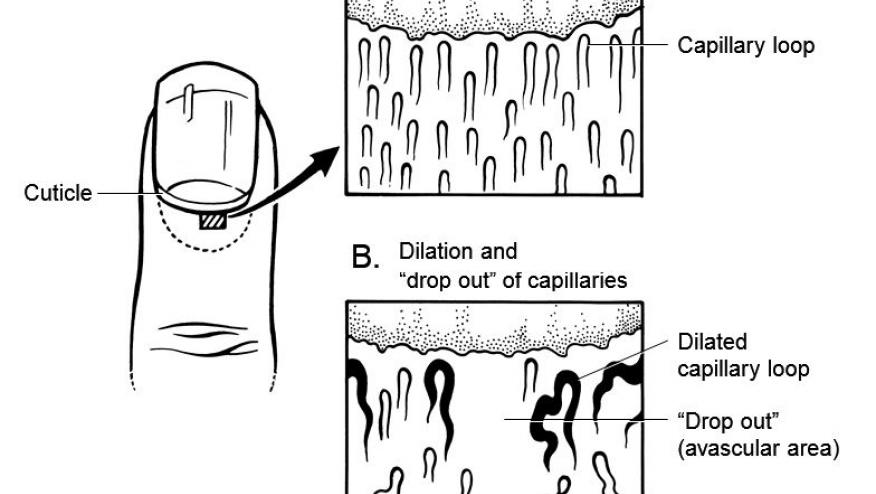
Capillaroscopy is a non-invasive imaging technique used for the in vivo assessment of the microcirculation. It can be performed using various optical instruments, but only the dermatoscope and videocapillaroscope have demonstrated good validity and inter- and intra-observer reliability. At present, only the videocapillaroscope has commercially available software to allow a standardized approach in the analysis of capillaries. Skin capillaries at the nailfold are evaluated because the fingers are involved in pathological processes such as Raynaud’s phenomenon.
Several abstracts and sessions on nailfold capillaroscopy (NFC) were presented during the conference.
A retrospective study by Dr. Alberto Sulli and colleagues compared NFC findings among patients with limited and diffuse cutaneous systemic sclerosis (SSc). Their cohort consisted of 157 patients, majority of whom had SSc (127) and 30 patients with primary Raynaud’s phenomenon. Capillary loss were seen in both limited and diffuse SSc patients while higher B scores, capillary density and abnormal shapes were associated more with diffuse SSc. In addition, the study also showed a significant association of the “late” scleroderma pattern with diffuse SSc.
In their study, Dr. Valera-Ribera et al. (abstract 2459) analyzed the association between NFC at the time of diagnosis of systemic sclerosis and major adverse cardiovascular events (MACE) and mortality on follow-up. Their results show avascular areas on NFC was an independent risk factor for all-cause mortality from all causes including SSc. Meanwhile, hemorrhages seem to show a protective effect. Additional studies may be required to elucidate robust evidence; however, these findings reinforce the value of NFC as a diagnostic tool in SSc.
In one of the scientific sessions, Dr. Smith discussed the potential role of NFC in ILD. She highlights studies showing that the “scleroderma pattern” in NFC was able to distinguish between CTD-ILD and IIPs. These findings highlight the importance of closer monitoring of ILD patients particularly because it may be the initial presentation of a CTD and that NFC can be considered an additional tool for diagnosis.
During the last day of the meeting, Dr. Maurizio Cutolo gave a very informative talk on the value of capillaroscopy in rheumatology to a full audience. He reviewed the evidence supporting the utility of NFC in the assessment of microvascular damage in SSc highlighting the recognition of a “scleroderma pattern” that can distinguish between primary and secondary Raynaud’s phenomenon. In addition, detection of this pattern may indicate an underlying CTD like systemic sclerosis. The identification of these early changes - few giant capillaries and/or microhemorrhages promote early diagnosis that greatly impacts disease outcomes among patients. Dr. Cutolo further discusses other NFC patterns seen in other CTDs such as the “combe-like” pattern observed in patients with APS and overlap syndromes as well as the “scleroderma-like” pattern in patients with dermatomyositis and MCTD. Additionally, Dr. Cutolo presented the standardized description of what is seen by capillaroscopy by the EULAR study group on microcirculation in Rheumatic Diseases/SCTC Consensus. He describes the fast-track algorithm that helps categorize a non-scleroderma vs. scleroderma pattern according to capillaroscopic findings like density, dimensions, abnormal morphology and hemorrhages.
The value of nailfold capillaroscopy extends beyond the characterization of the microcirculation to its use in clinical practice. As clinicians, patients with rheumatic diseases present with a variety of signs and symptoms and at different timeframes of their disease (early vs. late). Use of additional diagnostic tools, in this case nailfold capillaroscopy, allows for earlier diagnosis in patients presenting with Raynaud’s phenomenon, reinforcing the importance of close follow-up particularly in patients with unspecified ILD or even a guide for CV risk screening.
References:
Smith V. et al. Best Pract Res Clin Rheumatol. 2023 mar; 37(1): 101849
Smith V, et al. Rheumatology. 2022; 61(6):2217-2220






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.