

EGPA Review Save


Know-it-now
- EGPA diagnosis requires synthesis of clinical, laboratory, imaging, and histologic data; there is no diagnostic test or definitive biomarker.
- Phenotype-oriented classification (eosinophilic vs vasculitic) is central to modern therapeutic decision-making.
- Management is shifting away from glucocorticoids to using targeted biologics that are GC--sparing.
- Severe, organ-threatening disease mandates conventional immunosuppression guided by vasculitic involvement.
A current review of eosinophilic granulomatosis with polyangiitis (EGPA) provides current recommendations on diagnosis and management.
EGPA is a rare, heterogeneous immune-mediated disease characterized by variable combinations of eosinophilic inflammation, asthma/airway disease, and systemic vasculitis. The 2026 expert perspective published in Frontiers in Immunology provides a contemporary synthesis of diagnostic challenges and a phenotype-oriented management strategy, moving beyond a one-size-fits-all, glucocorticoid-centric paradigm toward individualized care grounded in disease biology and organ involvement.
Diagnostic approach
The diagnosis of EGPA remains challenging because no single biomarker captures the full spectrum of EGPA. The authors emphasize the need for integrated clinical reasoning, combining:
- Clinical features: adult-onset asthma, sinonasal disease, peripheral neuropathy, skin and cardiac involvement.
- Laboratory findings: eosinophilia and inflammatory markers; ANCA testing with recognition that more than half of patients are ANCA-negative, often reflecting a more eosinophilic phenotype.
- Imaging and histopathology: used selectively to confirm vasculitis or eosinophilic tissue infiltration where feasible.
The review underscores early recognition and multidisciplinary assessment (rheumatology, pulmonology, neurology, cardiology) as central to avoiding diagnostic delay and irreversible organ damage.
Phenotype stratification
Importantly, the clinician must distinguish whether the EGPA manifestations are eosinophilic-dominant and vasculitic-dominant, as this has therapeutic implications. ANCA-positive disease more commonly associates with classic small-vessel vasculitis features, while ANCA-negative disease often exhibits prominent eosinophilic tissue infiltration, asthma, and cardiac involvement. This stratification supports tailored therapy rather than rigid adherence to historical algorithms.
Therapeutic management
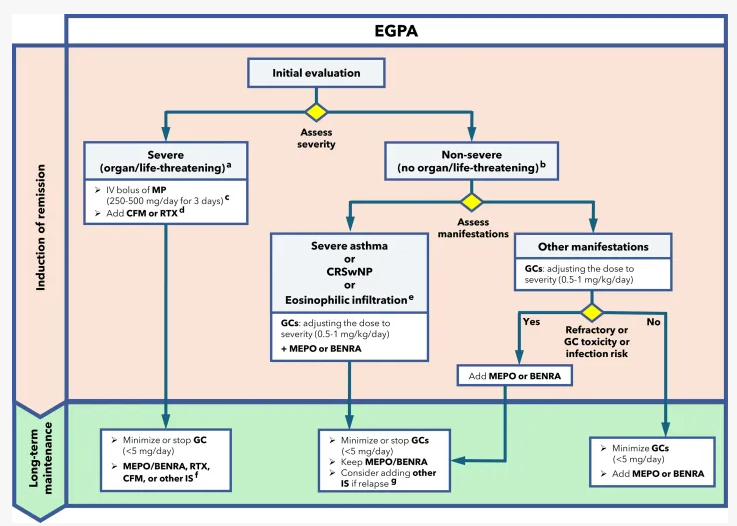
EGPA treatment has progressed toward glucocorticoid-sparing strategies. While systemic glucocorticoids remain fundamental for induction, long-term toxicity necessitates early planning for minimization.
- Non–organ-threatening disease: Anti–IL-5 or IL-5 receptor biologics are highlighted as effective options to control eosinophilic activity, reduce relapse risk, and facilitate steroid tapering, particularly in asthma-predominant or relapsing disease.
- Organ- or life-threatening vasculitis: Conventional immunosuppressants remain essential. Cyclophosphamide or rituximab are discussed in the context of severe vasculitic manifestations, with treatment intensity guided by organ involvement rather than eosinophil burden alone.
The review provides pragmatic recommendations on sequencing therapies and balancing efficacy with cumulative toxicity, aligning treatment selection with disease severity and dominant phenotype. [frontiersin.org]
A notable strength of the article is the presentation of a structured treatment algorithm designed to support day-to-day clinical decision-making. This framework integrates disease severity, organ involvement, and eosinophilic versus vasculitic predominance, aiming to standardize care while preserving flexibility for individualized management.
The chronicity of EGPA mandates, individualized multidisciplinary are with monitoring aimed at disease activity reduction, adverse effects avoidance, asthma control, and limiting cumulative glucocorticoid exposure.
Join The Discussion
Thank you
Disclosures
Disclosures
The author has no conflicts of interest to disclose related to this subject
The author used AI to research and organize this content, and maintains responsibility for its accuracy






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.