

Tocilizumab vs. Methotrexate in Rheumatoid Arthritis Save


A large randomized rheumatoid arthritis (RA) clinical trial compared subcutaneous tocilizumab (TCZ) vs oral methotrexate (MTX) vs. the combination of subcutaneous TCZ and MTX, and showed that TCZ was superior to MTX, either given as TCZ monotherapy or in combination with MTX.
To evaluate the efficacy and safety of subcutaneous tocilizumab monotherapy, tocilizumab-methotrexate, and methotrexate alone for patients with RA.
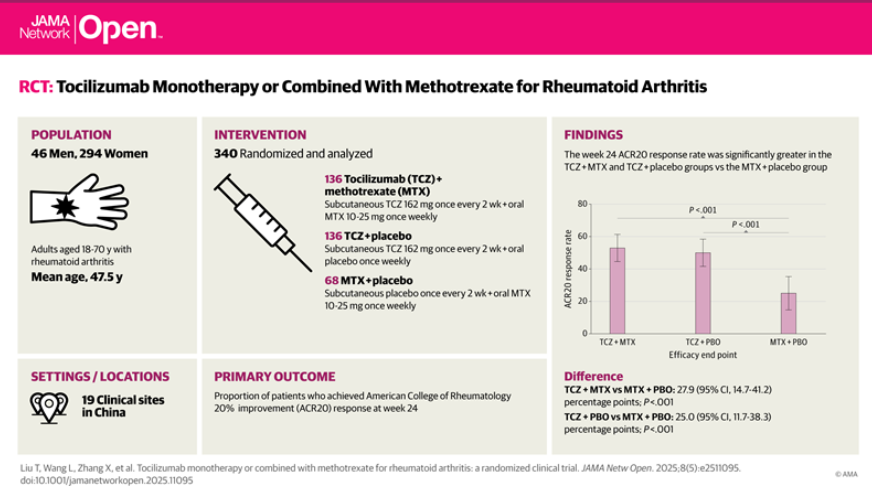
This double-blind, large-scale phase 3 randomized multicenter clinical trial from China enrolled a total of 340 adult RA patients (with an inadequate response to csDMARDs) in a 24-week double-blind treatment phase, a 24-week extension phase, and 8 additional weeks of safety follow-up. Patients were randomized 2:2:1 to either MTX-placebo (PBO), or TCZ-PBO, or TCZ-MTX. The primary endpoint was the percentage of those achiving a ACR20 response at week 24. At week 24, patients achieving a DAS28) <3.2 continued their double-blind treatment; while those with a DAS28 > 3.2 received open-label TCZ-MTX. Ssbcutaneous TCZ (162 mg) was given once every 2 weeks; and oral MTX (10-25 mg) was given once weekly.
The study population was mostly women (86.5%) with a mean age of 47.5 years. The week 24 ACR20 response rate significantly (P < .001) favored the TCZ-MTX group:
- TCZ-MTX - 52.9%
- TCZ-PBO - 50.0%
- MTX-PBO - 25.0%
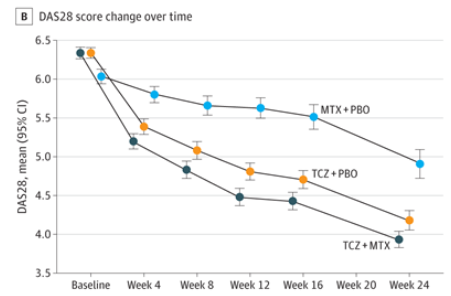
At week 48, responders on TCZ-PBO or TCZ-MTX maintained efficacy out to week 48. And week 24 nonresponders who were switched to TCZ-MTX improved disease status. No new safety signals were observed for tocilizumab.
While equivalent efficacy was seen for TCZ monotherapy and TCZ-MTX combo therapy, these were superior to MTX monotherapy.
Join The Discussion
I don’t see the above as equivalent efficacy of monotherapy TCZ vs combination. The DAS graph above, while not powered to show differences, shows clear trends (based on confidence intervals) that combo did work better than mono. I agree this is some of the best monotherapy data available, but MTX seems to add something in particular potentially for deeper responses which would account for the differences in absolute DAS without seeing a difference in ACR20.
AB. All valid points. But 2 things to temper the 1st look interpretation.
1. The primary endpoint was the ACR20 - not the DAS
2. The DAS28 differences were not significant between TZC-PBO and TCZ-MTX
But I agree with you, in that these results strengthen my impressions of TCZ and how it should be used......JC
Keep in mind that the secondary endpoint of ACR 50 response was also reached in the TCZ + MTX and TCZ monotherapy groups. The average MTX dose was around 11mg q week in both TCZ+MTX and MTX + Placebo groups. That may sound low compared to MTX doses used in the USA, but reducing the MTX when used in combination with TCZ may help reduce AE such as Leukopenia and LFT elevations. Overall a nice study.
"Patients were eligible for inclusion if they had received a diagnosis of RA (for ≥6 months), had received methotrexate (for ≥12 weeks) and experienced treatment failure of at least 1 csDMARD (including methotrexate)" citation from the paper. So, study addressing a non-naive, stablished (mean (SD) duration of RA=8.7(7.4)) RA population.....
Good pickup. The devil is in the details of the methods. Nonetheless, these pts, while not Rx-naive or MTX-naive, are real world..... Do with this as you wish! JC
Disclosures
Disclosures
The author has no conflicts of interest to disclose related to this subject






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.