

Screening High Risk Myositis Patients for Cancer Save

An Italian retrospective study of 411 idiopathic inflammatory myopathies (IIM) patients applied IMACS criteria to assess the risk of cancer and found significantly more cancers in those at high risk.
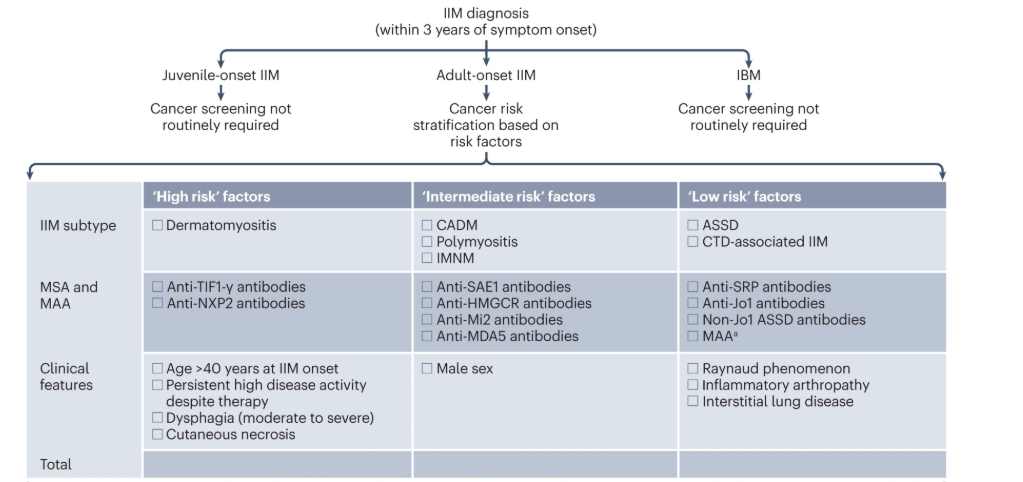
The 2023 International Myositis Assessment and Clinical Studies Group (IMACS) introduced a risk-stratification model for cancer screening in IIM patients. Their recommendations categorize cancer risk stratified into standard, moderate or high risk according to the IIM subtype, autoantibody status and clinical features. Also these recommendations outline a ‘basic’ screening panel (including chest radiography and preliminary laboratory tests) and an ‘enhanced’ screening panel (including CT and tumour markers). Third, the recommendations advise on the timing and frequency of screening via basic and enhanced panels.
Previously these cancer screening recommendations were studied in a prospective adult cohort of 370 dermatomyositis patients from the University of Pennsylvania rheumatology-dermatology division (2008-2024). Based on the IMACS stratification, patients were classified as: 54% high risk, 37% intermediate risk, and 9% low risk. While 18/370 (~5%) developed a malignancy, 83% came from the high risk group and 17% came from the intermediate risk group (none from low-risk patients).
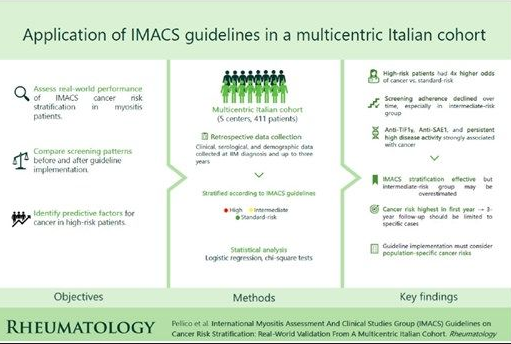
The current study aimed to evaluate the effectiveness of IMACS-based risk stratification in predicting malignancy and assess adherence to cancer screening recommendations in a multicentric Italian IIM cohort.
This retrospective multicenter study included 411 IIM patients; 44% were classified as high-risk, 38% intermediate-risk, and 18% were standard-risk. Cancer was diagnosed in 9.2% of patients within three years of IIM onset. Cancer was more likely with:
- High-risk (OR = 4.05, p= 0.026)
- Anti-TIF1γ (OR = 12.3, p< 0.001)
- anti-SAE1 (OR = 11.9, p= 0.012)
- SAE1: anti-small ubiquitin-like modifier 1-activating enzyme subunit 1 (SAE1) antibodies
The IMACS stratification model effectively predicts cancer risk in IIM. However, real-world screening practices show inconsistencies, particularly in intermediate-risk patients. The need for cancer screening can be guided by these IMAC categorizations, but there is inconsistent predictability in intermediate risk individuals. Refinement of current guidelines should be based on real-world data and prospective studies.
Lastly, should cancer risk workups (potentially invasive, expensive and tested in IIM) be guided by serologies alone? Also little is known about the application of newer blood tests and screens for cancer (CancerGuard, GRAIL, GALLERI, MCED), and what their role is outside of age-appropriate screening. The American Cancer Society states these tests are not intended to replace standard cancer screenings (e.g., mammograms, colonoscopies) and do not catch every type of cancer.
IMACS Screening Recommendations
.
ADD THE FIRST COMMENT
Disclosures
The author has no conflicts of interest to disclose related to this subject






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.