

DMARD Efficacy in RA-ILD Save


Know-it-Now
- MTX is not dangerous in RA-ILD patients — it had the lowest predicted mortality.
- Abatacept + MTX may be strongest in slowing ILD progression (but this is observational data; may have a reporting bias)
- Antifibrotics (nintedanib, pirfenidone) reliably slowed FVC decline
- JAK inhibitors show good drug retention (81.7%) but potential safety signals
- Evidence provided is at best low-to-very-low certainty
A network meta-analysis in the Journal of Autoimmunity reviews the pharmacologic options for rheumatoid arthritis–associated interstitial lung disease (RA-ILD). RA-ILD guidelines were recently presented by ERS/EULAR, but these were mainly conditional, low-certainty recommendations.
Eligible studies comprised RCTs and high-quality observational comparative studies enrolling adults with RA-ILD, confirmed by HRCT or other imaging modalities. The metanalysis included 27 studies (only 2 RCTs; 8,186 patients) that covered 14 regimens — methotrexate (MTX), abatacept (with and without MTX), TNF inhibitors, tocilizumab, rituximab, JAK inhibitors, cyclophosphamide, nintedanib, pirfenidone, leflunomide, tacrolimus, azathioprine, mycophenolate, and iguratimod combinations. This Bayesian random-effects NMA examined mortality, ILD progression, adverse events, FVC%, and treatment retention.
The major limitation of this report was that 25 of 27 studies were observational, evidence certainty was graded low-to-very-low across nearly every outcome (CINeMA), and most treatment comparisons rested on only 1–2 direct studies — meaning indirect estimates carry substantial uncertainty. The authors explicitly label their findings "hypothesis-generating," not practice-changing.
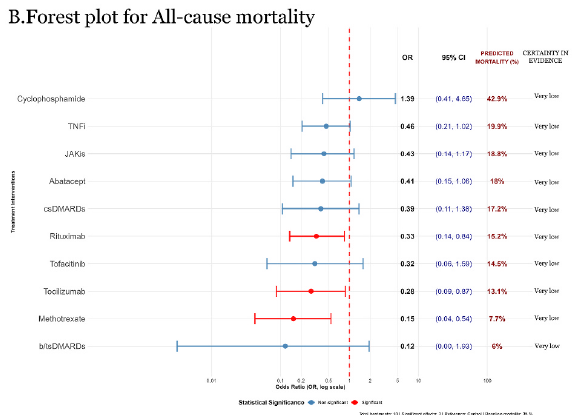
Mortality
MTX had the lowest predicted all-cause mortality (7.7%; OR 0.15), followed by tocilizumab (OR 0.28) and rituximab (OR 0.33). This argues against MTX's historical reputation for pulmonary toxicity — but the authors are careful to frame it as likely confounded by indication (healthier, less severe ILD patients probably received MTX) rather than proof of a protective effect.
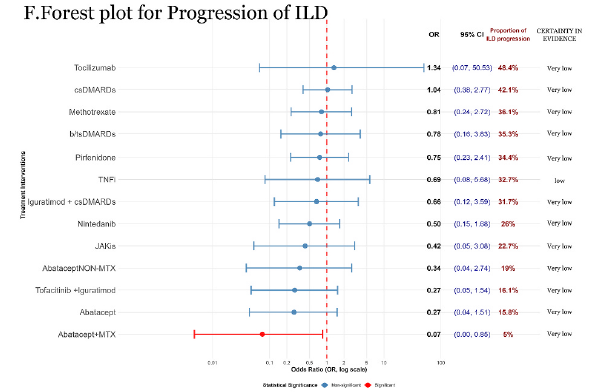
ILD progression
Abatacept + MTX stood out, cutting progression risk by roughly 93% (OR 0.07) versus control — the single most striking point estimate in the paper, attributed to complementary T-cell costimulation blockade and MTX's broader anti-inflammatory action. Again, this rests on sparse observational data.
Lung function (FVC%)
Antifibrotics performed as expected — nintedanib and pirfenidone both showed significantly slower FVC decline (MD +2.20 and +2.18, respectively), consistent with their RCT pedigree (INBUILD, and the pirfenidone phase 2 trial). Immunoglobulin showed the largest FVC% signal (MD +13.59) but from only one small study.
Tolerability
JAK inhibitors had the best retention (81.7%) and lowest discontinuation rate (7.9%) — but came with a numerically higher rate of serious adverse events, including ICU admission and respiratory failure (44.7% absolute incidence), reinforcing that low discontinuation isn't synonymous with safety in this population. Azathioprine and csDMARDs fared worst on tolerability, largely due to cytopenia, infection, and hepatotoxicity.
Bottom line for clinic: This NMA doesn't overturn ERS/EULAR guidance, but supports antifibrotics for progressive fibrosing phenotypes, offering a data-driven rationale to reconsider MTX in selected RA-ILD patients, flagging abatacept + MTX as a reasonable option for progression-prone patients (with close infection/cardiovascular monitoring), and positioning JAK inhibitors as an option for poor treatment tolerators without high infection risk.
Prospective, ILD-subtype-stratified RCTs remain the clear unmet need.
ADD THE FIRST COMMENT
Disclosures
The author has no conflicts of interest to disclose related to this subject
The author used AI to research and organize this content, and maintains responsibility for its accuracy






If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.