EULAR has published a "points to consider" (PtCs) guidance on the development of criteria for the assessment of the disease activity in adult-onset Still’s disease (AOSD).
AOSD can be challenging to diagnose, owing to a lacking clear pathogenic cause. It may also challenging to monitor, treat or know when to stop antiinflammatory therapy as there is no clear biomarker upon which to make such decisions. Having consensus guidance on how to quantitate the systemic or articular activity of AOSD, would have a significant influence on optimal management of patients and the development of clinical trials addressing therapy and outcomes.
Currently there is no consensus on how to best assess AOSD activity; nor are there validated tools developed on reasonably large patient data sets. The current PtC review follows the 2024 publication of the EULAR/Paediatric Rheumatology European Society (PReS) Recommendations on diagnosis and management of children and adults under the common umbrella of the unique name of Still’s disease [
2]
A EULAR task force consisted of 23 members from 7 different European countries, and none from North America or Asia. Following a literature review, three Delphi exercises resulted in 3 overarching principles and 11PtCs. The purpose of this exercise was to establish a clear definition of AOSD and AOSD disease activity that might help guide therapy or identify refractory patients. These proposed PtC will need to be validated in a real world setting and cohort.
The authors aim to develop a clinical tool that is reliable, and easily applied, to improve patient management and outcomes.
Overarching Principles
- NEED: The importance of an appropriate definition for the disease activity to specifically manage patients with AOSD is recognised
- AIM: The criteria for the assessment of disease activity for AOSD have to be valid, reliable, and easily transferable in any clinical setting
- SCOPE: The development of specific criteria for the assessment of disease activity should include a precise definition of the clinical features which could better describe the patient condition.
Points to Consider
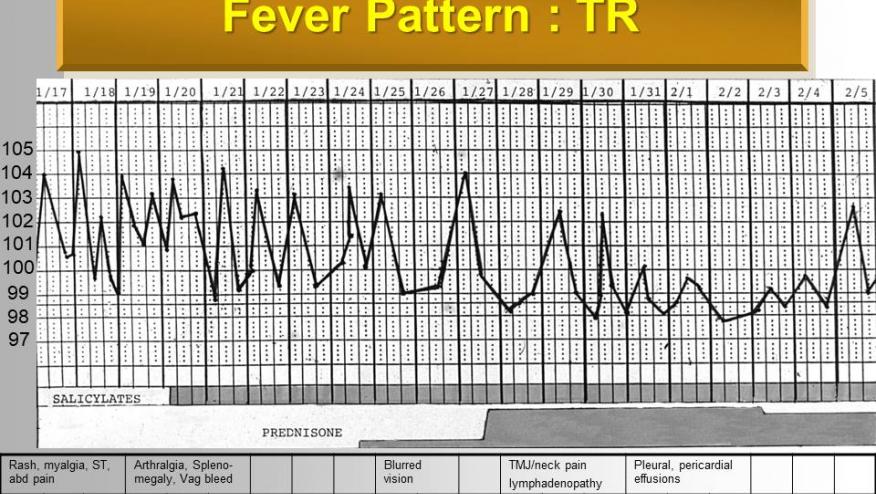
- Fever (being most frequent clinical sign of disease activity in AOSD) has to be considered as one of the variables of the core set.
- Skin rash, although evanescent, may occur at the onset of the disease and during its flares
- Arthralgia and arthritis are seen in a large majority of patients with AOSD at the onset of the disease and during its flares
- The systemic involvement of AOSD may affect different organs, resulting in secondary lymphoid structures enlargement and serositis, which can be observed in more severe patients
- Hyperferritinaemia is the laboratory marker most frequently associated with AOSD onset and relapses
- Increased levels of CRP and ESR, although nonspecific, are commonly detected during AOSD onset and may be helpful in identifying a clinical flare
- Increased levels of liver enzymes are frequently associated with AOSD systemic involvement
- Increased white blood cell count, mainly polymorphonuclear cells, is commonly detected at the onset of the disease and may be helpful in identifying a clinical flare
- Patient global VAS may be a helpful criterion to assess AOSD disease flare
- An objective definition of ‘remission’ is an important need, together with the definition of disease activity, to identify the clinical therapeutic target to be reached in patients with AOSD
- The development of a disease-specific PRO may improve the management of AOSD by incorporating the patient perspective
This EULAR PtC exercise has successfully highlighted the many, impressive, but protean features that have defined AOSD since the original description by Bywaters in 1971 and Bujak, et al in 1973. These PtC represent a consensus and preferred inclusion of criteria that could be developed into an "activity" or severity score. That would be the logical next step.
(Editors comments: 1) Hyperferritinemia is not the most frequently found inflammatory marker in AOSD onset or relapses, as it is seen in roughly 50% of AOSD patients with active systemic disease. Better performance is seen with elevated ESR or CRP, that can be seen in 85-95% of AOSD patients at the onset or during flares; 2) While PRO's would be a very welcomed parameter to follow in AOSD, there is very little quality data regarding Patient Global VAS or any other disease specific PRO that would be useful in patient assessment or management. Nevertheless, a patient perspective on disease severity or impact would be welcomed. 3) Remission needs to be defined, with an emphasis on whether this is remission on therapy vs. off therapy and whether remission on therapy would be reasonably predictive of future remission off therapy, that would be sustained and long-lasting.)









If you are a health practitioner, you may Login/Register to comment.
Due to the nature of these comment forums, only health practitioners are allowed to comment at this time.